
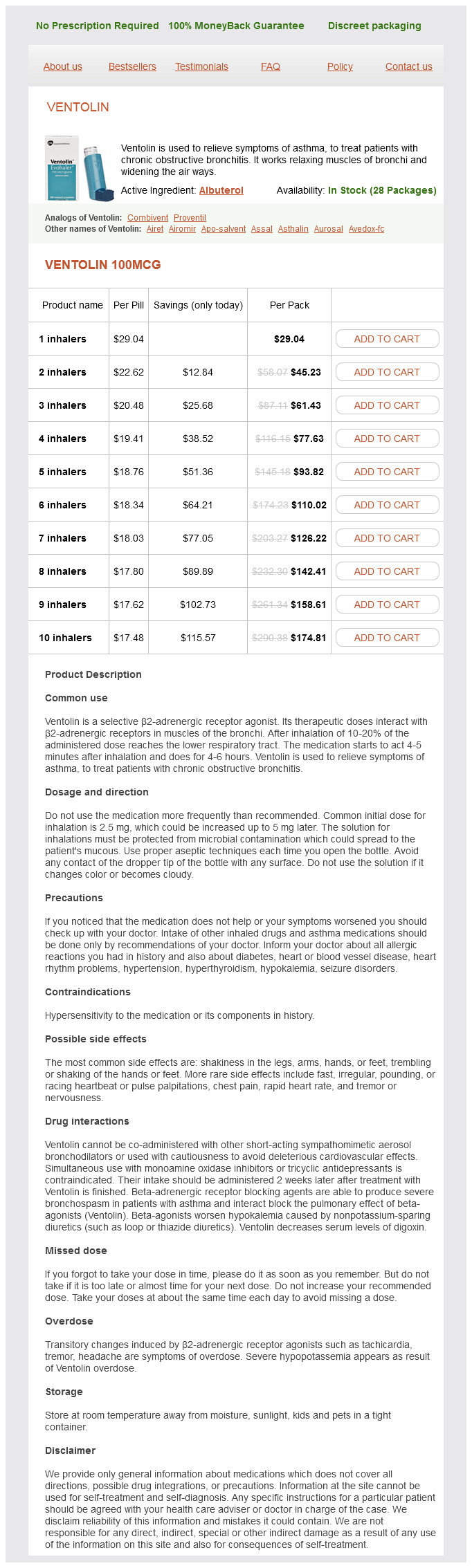
Albuterol dosages: 100 mcg
Albuterol packs: 1 inhalers, 2 inhalers, 3 inhalers, 4 inhalers, 5 inhalers, 6 inhalers, 7 inhalers, 8 inhalers, 9 inhalers, 10 inhalers
In stock: 686
Only $18.57 per item
It is possible to achieve over 50% overall 5-year survival rate in recurrent gynecologic cancers with exenterative surgery [14] asthma treatment long-term 100 mcg albuterol buy free shipping. However, it is associated with high morbidity (3050%) and mortality (810%), and is therefore usually offered when other modalities of treatment like radiotherapy and chemotherapy are no longer suitable options. Pelvic exenteration was first described by Brunschwig [5] in 1948, when it was performed for palliation of symptoms. The operation later evolved into a potentially curative intervention for patients with central recurrences. Over time, the indications for exenteration have extended to pelvic sidewall recurrences whenever resection with clear margins is achievable [6]. Effective preoperative assessment by expert teams working in cancer centers is paramount to ensure patients are appropriately identified for exenteration, and outcomes are optimized. Informed consent and extensive counseling are essential elements of management to ensure patients are fully aware of the potential risks associated with this surgery. Pelvic exenteration involves radical excision of the uterus in conjunction with the adjacent viscera from the urologic or rectal compartments. When surgical excision extends to all the three compartments (bladder, uterus and rectum), it is referred to as total pelvic exenteration. In cases where the lower third of the vagina is not involved, an attempt to conserve the lower vagina, perineal body, and anal canal is appropriate. This is referred to as supra-levator pelvic exenteration as it does not include the excision of levator ani muscles. Pelvic exenteration is associated with diversion procedures for urine (Chapter 149) and feces (Chapter 37). Rectal excision is usually associated with a colostomy except where it is feasible to perform low anorectal anastomosis. However, many patients may have had prior radiation, and in such patients low anorectal anastomosis is associated with high anastomotic leaks and therefore a colostomy is favored. Management the extent of exenterative surgery is tailored to tumor profile and is aimed to achieve clear excision margins. Exenteration involving total colpectomy (removal of vagina) extends below the levator Case selection for pelvic exenteration Careful case selection is essential. After having excluded non-surgical options (chemotherapy and radiotherapy), exenterations should only be offered to well-motivated patients who understand the surgical morbidity and consequences of the procedure on their Gynecologic and Obstetric Surgery: Challenges and Management Options, First Edition. Depending on the excision margins, one may obtain total microscopic clearance (referred to as R0), margins with macroscopic clearance but microscopic involvement (referred to as R1), or margins with macroscopic and microscopic involvement (referred to as R2). Compared with R0, R1 has a poorer prognosis and R2 has the least favorable prognosis. A careful assessment is undertaken of the disease distribution and plans are made for the extent of surgery. The latter is performed usually in cases with malignant fistulae or impending bowel obstruction. Contraindications for exenteration Leg pain, lymphedema, and hydronephrosis were regarded as the classic triad of doom and were contraindications for exenterative procedures as they signified nerve involvement, lymphatic involvement, or lateral pelvic sidewall extension, respectively.
Hogweed (Canadian Fleabane). Albuterol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96267
Surgical technique the pelvis and abdomen are thoroughly explored to rule out peritoneal disease asthma symptoms kid 100 mcg albuterol order otc. The retroperitoneal spaces on the pelvic sidewalls are then entered by division of the round ligaments. The lymph-bearing tissue along the pelvis is then evaluated for obvious metastatic disease. The pararectal and paravesical spaces are developed, followed by identification and transection of the uterine vessels at their point of origin from the internal iliac vessels. The bladder is then mobilized from the anterior vagina, allowing for adequate resection of a 2-cm vaginal cuff. The parametrial tissue is dissected and brought over the ureters, which are dissected to the point of their insertion into the bladder bilaterally. The cervix and uterus are now free of all their vascular and suspensory attachments and can be removed. Management of lymph nodes Metastatic disease in clinically positive or enlarged pelvic lymph nodes cannot be cured by surgery alone, and women with this condition will require postoperative radiation. If the diseased lymph nodes had been discovered preoperatively, such patients would not have been offered primary surgery. Although modern surgical and radiotherapy techniques have minimized risks, complications may be more common when both surgery and radiation are used, compared with a single modality of treatment. The ideal management of enlarged suspicious lymph nodes found at the time of radical surgery is controversial. The first option available to the surgeon is to send the suspicious lymph nodes for frozen-section histologic assessment and abandon the procedure Management preparation Mechanical bowel preparation and the use of heparin can be considered on the day before the surgery. However, the unavailability of the frozen-section technique, and its sensitivity and specificity for assessment of lymph node metastases do not make it a universal option. The second alternative is to complete the pelvic lymphadenectomy and obtain a formal histologic assessment, planning the radical hysterectomy as a second-stage procedure if the lymph nodes are negative. This approach allows for ultra-sectioning of the lymph nodes, with higher sensitivity and specificity for detecting lymphatic metastases. Nevertheless, a second anesthesia and operative procedure are not without morbidity. Inevitably, some degree of scarring and adhesions will develop on the pelvic sidewall, making the second procedure challenging. The last option is to fully complete the lymphadenectomy and radical hysterectomy, with adjuvant radiotherapy offered should the lymph nodes be positive on final histology examination.
Intraoperatively asthma treatment plan student order 100 mcg albuterol with mastercard, care should be taken to identify the correct layer for dissecting the bladder off the lower uterine segment. I personally do not insert a Foley catheter until after I have entered the anterior cul de sac and clamped the uterine vessels bilaterally. This interesting anatomic variation leads to the posterior cul de sac being multiple centimeters above the external cervical os while the bladder reflection can be in very close proximity to the external os. The surgeon must remember that the ureters can be pulled down along the lateral cervix as the uterus prolapses, putting them at risk of ligation, especially in cases of cervical hypertrophy. The anterior cul de sac is typically not entered until multiple tissue bites have been taken. If continued difficulty is encountered in identifying the peritoneal reflection, the uterus may be bisected (preferably along its posterior surface) once the surgeon is confident that the uterine arteries have been ligated. Amputations of the long cervix may be needed to allow better traction on the uterus. If this maneuver is performed, the surgeon must be certain to maintain traction on the proximal cervical stump in order to not lose anatomic orientation. If the mass cannot be removed as an intact cyst, the fluid can be aspirated but only if the visual appearance is that of a completely benign cyst. Fortunately, experienced surgeons can remove most adnexae (when planned) vaginally (see Chapter 112). After completing the removal of the uterus, I typically grasp the ovary with a Babcock clamp and gently massage its base to help it descend as much as possible. Thick omental or bowel adhesions obliterating the posterior cul de sac can be very problematic, and make posterior entry difficult. The surgeon should refrain from cutting through omentum-like fatty tissue as it can be very vascular. Thick adhesions in the anterior cul de sac are typically the result of cesarean section, as discussed earlier. However, the surgeon must be ready to deal with the reduced vaginal caliber and lack of uterine descent. Performing a large episiotomy can enlarge a restricted introitus, but more importantly shorten the posterior vaginal wall and bring the cervix closer to the introitus. Methodical traction on the uterus, and directed massage of the uterosacral and cardinal ligaments, can further bring the uterus closer to the introitus. Practice patient positioning in the office can indicate whether intraoperative positioning will be comfortable for the patient.
Syndromes
Additional information:
Usage: ut dict.
Tags: 100 mcg albuterol purchase, cheap albuterol 100 mcg buy, discount albuterol 100 mcg mastercard, discount albuterol 100 mcg on-line
Rasarus, 48 years: After cleaning with a sterile medium, a fluid collection drape should be placed under the pelvis to facilitate the measurement of fluid balance. Classification of hemorrhagic shock Hemorrhagic shock can be classified into four groups Table 40. Non-absorbable sutures theoretically decrease the risk of adhesions in the uterine cavity, but with the risk of leaving a "foreign body" in the uterine cavity.
Cyrus, 46 years: Grade 0 and I fibroids are easier to resect as the majority of the fibroid is visible within the uterine cavity. In situations where there is uncertainty about the tissue origin of a complex pelvic mass, the use of different panels of immunohistochemistry markers on biopsy specimens or ascitic cytology can be informative. Fortunately, necrotizing fasciitis is uncommon, but the mortality rate is high at approximately 2040%.
Sulfock, 29 years: Alternatively, placing the patient in the left lateral position with a slight head-down tilt may trap the embolism in the right atrium [8]. If the placenta is cut, the baby should be delivered immediately, and immediate cord clamping is essential to prevent fetal exsanguination. Secondary causes of hypertension, especially in the younger patient, should also be excluded.
Givess, 54 years: During gynecologic procedures, the bowel should be mobilized as necessary and packed away from the pelvis. Production Prior to birth, red blood cells are produced largely by the liver and spleen but, after birth, production occurs only in the red bone marrow (myeloid tissue). However, this patient preferred to have a chance of amenorrhea, which is more likely with a concomitant endometrial ablation.
Zakosh, 47 years: Although each muscle has its own action, these muscles function as a coordinated group to enable eye movements. It may cause severe pain and an outward bulging of the tympanic membrane due to accumulated fluids. These instruments work by receiving energy from a generator (the same generator used for monopolar devices).
Tragak, 37 years: The sigmoid is at risk during mobilization to identify the left ovarian vessels and ureter. A Foley catheter tied tightly around the uterus acts as an excellent tourniquet, and the uterine or internal iliac artery can be clipped or sutured. In the case of fistula occurrence after gynecologic surgery, it is appropriate to wait 612 weeks to allow suture dissolution and granulation tissue ingrowth, which can increase the chances of successful repair.
Sinikar, 34 years: Artery Vein Valve Endothelium of tunica intima Areolar connective tissue of tunica intima Tunica media Capillaries Arterioles connect with capillaries, the most numerous and the smallest blood vessels. Background A child may need laparoscopic surgery for ovarian masses, appendectomy, cholecystectomy, splenectomy, abdominal exploration in trauma, and operations for uterovaginal abnormalities. The Black Death is the largest known pandemic (large infectious outbreak), which killed about half of the population of Europe (estimated at up to 200 million people worldwide) from 1347 to 1351.
Rhobar, 40 years: Appropriate broad-spectrum antibiotics are given to treat the associated infection. Two opposing sphincters forces determine the movement of fluid between capillary blood and interstitial fluid: osmotic presCapillary Capillaries network sure and blood pressure. The provision of contraception to a young person less than 16 years of age has been much discussed in the literature.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





