
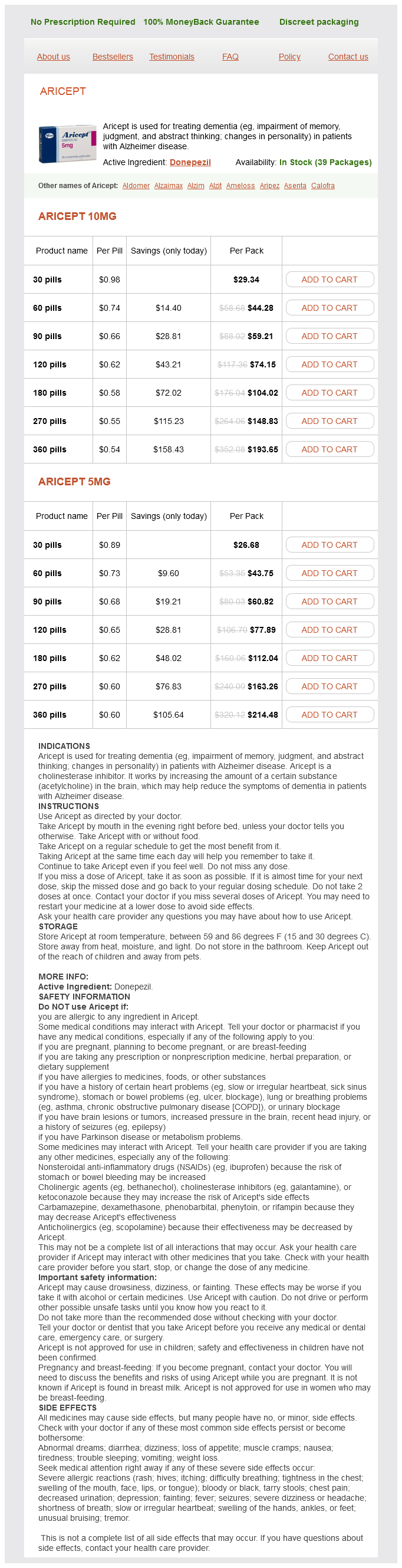
Aricept dosages: 10 mg, 5 mg
Aricept packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 593
Only $0.63 per item
Four histologic types of adrenal cysts have been described: pseudocysts medicine 4h2 discount 10 mg aricept visa, endothelial cysts, epithelial cysts, and parasitic cysts. Adrenal pseudocysts do not possess a cellular lining and are believed to be the result of previous intraadrenal hemorrhage or infarction in most cases. Endothelial cysts lack proliferating endothelium and include lymphangiomatous and angiomatous subtypes. Epithelial cysts are lined by a true epithelium and can be further characterized as glandular cysts, embryonal cysts, and cystic adenomas based on pathogenesis. Parasitic adrenal cysts may occur in association with disseminated Echinococcus infections; however, it is extremely rare for a parasitic adrenal cyst to be the only site of infection (Otal et al, 1999; Guo et al, 2007; Wedmid and Palese; 2010). It can be difficult to distinguish a benign adrenal cyst from cystic adrenal neoplasms. This is especially true of adrenal neoplasms with associated hemorrhage or cystic degeneration, which may radiographically resemble an adrenal pseudocyst. Furthermore, 6 of the 7 adrenal neoplasms in this series were associated with adrenal pseudocysts. A review of multiple series accounting for 515 adrenal cysts noted that 7% of the lesions were associated with malignancy, all of which were pseudocysts (Neri and Nance, 1999). In addition, cases of cystic adrenal carcinoma and pheochromocytomas have been reported (Rozenblit et al, 1996). Compared with benign cysts, cystic adrenal neoplasms tend to be larger (>7 cm) and have thicker walls. In considering the reported incidence of malignancy associated with adrenal cysts, it should be noted that histology in most series is based on surgical specimens, so the incidence of malignancy may be overestimated because small radiographically benign lesions likely remain unresected. The prognosis and subsequent follow-up after resection of an adrenal cyst are dependent on histology. Benign adrenal cysts warrant follow-up to monitor potential reaccumulation, and warrant re-treatment if symptoms return. Adrenal cysts associated with malignancy require follow-up in accordance with the malignant histology detected. Symptomatic adrenal cysts should be surgically removed, whereas small nonfunctional asymptomatic lesions with benign radiographic appearance may be treated conservatively with regular follow-up. Although most adrenal cysts are diagnosed incidentally, some become large in size and are symptomatic on presentation. The origin of large adrenal cysts is often difficult to distinguish from other organs, including the kidney, pancreas, spleen, and liver (Otal et al, 1999). Although the majority of adrenal cysts are benign and nonfunctional, routine endocrinologic evaluation should be performed to exclude active lesions. Owing to the relative rarity of adrenal cysts, well-defined diagnostic criteria have not been established. The suggested radiographic criteria for diagnosing an adrenal cyst include a well-defined, sharply marginated mass of fluid attenuation without any evidence of enhancement. The presence of peripheral calcifications has been noted in 15% to 70% of adrenal cysts (Song et al, 2008).
Blue Sailors (Chicory). Aricept.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96136
Men have more clearly demarcated areas of muscular attachment symptoms 7 days after implantation order aricept 10 mg with mastercard, and women have smaller iliac fossa (MacLennan, 2012). When the pelvis is visualized in the standing position, the anterior superior iliac spine and pubic symphysis lie parallel to each other (Barber, 2005). The pelvic inlet faces anteriorly, which allows most of the pressure of the intra-abdominal and pelvic contents to be directed toward the bony pelvis rather than toward the muscles and the fascia. This is in contrast to the surgical anatomy, which is most commonly described in the lithotomy position. Outer stratum the rectal fascia is part of the inner stratum and covers the anterior and lateral rectal wall, vessels, and nerves forming part of Denonvilliers fascia. The intermediate stratum encases the uterus and supporting vessels and provides additional pelvic support. Most of the support of the pelvic organs comes from the retroperitoneal connective tissue derived from the intermediate stratum. The fascia attached to the uterus is referred to as the parametrium and that surrounding the vagina is the paracolpium (Wei and DeLancey, 2004). The transversalis fascia is part of the outer stratum and is continuous with the endopelvic and lateral pelvic fascia. The endopelvic fascia extends from the uterine artery down to where the vagina and levator ani fuse. The iliac fascia is also part of the outer stratum and covers the iliacus and psoas muscles. It attaches to the iliac crest and runs down to the tendinous arch (white line) and is continuous with the posterior portion of the inguinal ligament. The thickened band of the pelvic fascia that runs from the ischial spine to the pubic bone is called the tendinous arch or the arcus tendineus. It originates from the pubic bone laterally and is connected to the pubovesical ligament medially and the tendinous arch of the levator ani (Fritsch et al, 2012). The inferior pelvic fascia is continuous with the obturator fascia and fascia of the pudendal canal. The superior pelvic fascia arises from the outer stratum and the obturator fascia. The vesicovaginal space is contained by the adventitia of the bladder anteriorly and vagina posteriorly. The space ends where the vagina fuses with the distal urethra and at the vesicocervical ligament (fusion of the bladder with the vagina and cervix). The prevesical space is between the fascia covering the bladder and the endopelvic fascia behind the pubis. The retrorectal space is between the rectal fascia and transversalis fascia over the sacrum. Laterally there are the paravesical and pararectal spaces, which sit adjacent to their respective organs.
At a location that is two thirds of the distance between the pubis and the umbilicus symptoms 4 weeks pregnant purchase aricept 10 mg online, the arcuate line is formed, as all aponeurotic layers abruptly pass anterior to the rectus abdominis, leaving this muscle clothed only by transversalis fascia and peritoneum posteriorly. The rectus abdominis arises from the pubis medial to the pubic tubercle and inserts on the xiphoid process and adjacent costal cartilages. The muscle is crossed by three or four tendinous intersections that are firmly attached to the anterior rectus sheath; thus the muscle can be divided transversely without significant retraction. Paramedian incisions lateral to the rectus divide these nerves, cause atrophy of the rectus, and predispose to ventral hernia. Anterior to the rectus and within its sheath, the triangle-shaped pyramidalis muscle arises from the pubic crest and inserts into the linea alba. InguinalCanal the inguinal canal transmits the spermatic cord and the ilioin guinal nerve in the male. The external oblique muscle, which folds over at its inferior edge as the inguinal ligament, forms its anterior wall and floor. Above the pubic tubercle, the fibers of the external oblique aponeurosis split to form the lateral edges (crura) of the external inguinal ring. Transverse (intercrural) fibers bridge the crura to form the superior edge of the external ring. By dividing the intracrural fibers, the external oblique can be separated along its fibers to gain access to the cord. In addition, during the performance of transperitoneal laparoscopic or robotic radical prostatectomy, the medial umbilical folds are used as landmarks to guide the dissection of the bladder to expose the space of Retzius. The lateral umbilical fold contains the inferior epigastric vessels as they ascend to supply the rectus abdominis. Top, Above the arcuate line, the aponeurosis of the external oblique muscle forms the anterior sheath, and the transversus aponeurosis forms the posterior sheath. The internal oblique muscle splits to contribute to both the anterior and the posterior sheaths. Transversalis fascia, which lines the inner surface of the abdominal wall, forms the posterior wall of the canal. The cord structures pierce this fascia lateral to the inferior epigastric vessels at the internal inguinal ring. The internal inguinal ring lies midway between the anterior superior iliac spine and the pubic tubercle, above the inguinal ligament, and 4 cm lateral to the external ring. Fibers of the internal oblique and transversus abdominis arise from the iliopsoas fascia and inguinal ligament lateral to the internal ring and arch over the canal to form its roof.
Syndromes
Additional information:
Usage: t.i.d.
Tags: 5 mg aricept buy fast delivery, aricept 5 mg low cost, aricept 5 mg discount, aricept 10 mg order visa
Silas, 60 years: He reports his experience with 25 patients during a 4-year period as showing that bladder capacity increased more than 20% (values referred to a comparison to age-adjusted bladder capacity) and end-filling bladder pressures showed clinically significant decreases in 29% of patients. It is possible that the degradation of the channel might follow the filling of the bladder and that the changes in conductance of sodium may be a signaling factor for the bladder and micturition when it reaches capacity.
Achmed, 28 years: Marketing claims aside, whether there is any difference in the efficacy or side effect profiles of these individual agents remains a topic of controversy. Effect of bladder ischaemia/reperfusion on superoxide dismutase activity and contraction.
Xardas, 57 years: In addition to the nerve fibers, other impor tant structures in the lamina propria include interstitial cells (myofibroblasts) and microvasculature. Thus the cause of nocturia was found to be multifactorial and often unrelated to an underlying urologic condition (Weiss et al, 1998).
Bram, 38 years: Nevertheless, current recommendations suggest serum or urine metanephrine testing for all adrenal lesions (Grumbach et al, 2003; Young, 2007b). Immunity to nerve growth factor prevents afferent plasticity following urinary bladder hypertrophy.
Larson, 41 years: Robot assisted partial nephrectomy versus laparoscopic partial nephrectomy for renal tumors: a multiinstitutional analysis of perioperative outcomes. However, in a review of the literature, Bø and colleagues (2009) noted an absence of evidence for this type of training, and it remains controversial.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





