
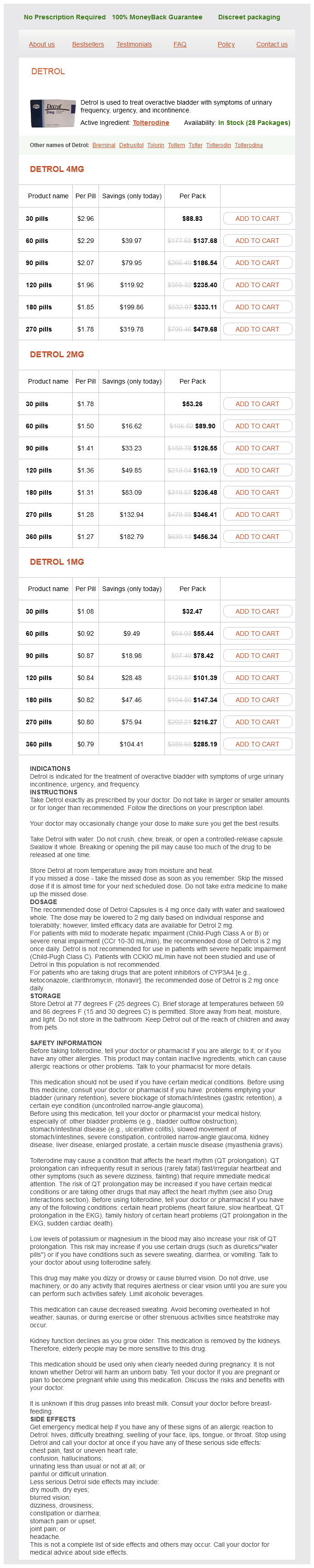
Detrol dosages: 4 mg, 2 mg, 1 mg
Detrol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 837
Only $0.84 per item
In some cases the disease may begin in the synovium (synovial tuberculosis) but spreads quickly to involve the articular cartilage and bone (articular tuberculosis) keratin intensive treatment detrol 1 mg low cost. A progressive pattern of destruction of the hip occurs in patients who are not treated. Diffuse form the disease may be active or inactive Look for periarticular erosions on radiographs A diffuse mass may be present on examination. Clinical features There is an insidious onset with aching in the groin and thigh and limp. The leg is scarred and thin, and shortening is often severe because many factors can contribute (adduction deformity, bone destruction, damage to the upper femoral epiphysis). There may be a lytic lesion involving either the head of the femur or the acetabulum. The outline of the articular ends of the bone becomes irregular because of destruction by the disease process. Radiology Radiographs show cysts on both sides of the joint and are not confined to the weightbearing areas. Arthroscopic synovectomy or open synovectomy is viewed as the treatment of choice for the active form of diffuse disease. Skin traction in a Thomas splint Provides rest of the affected part Relieves muscle spasm Prevents and corrects deformity Maintains joint space Minimizes chances of developing a wandering acetabulum. Joint arthroplasty:82 joint arthroplasty is not performed in the active stage and should only be considered after a safe period of absolute disease quiescence. Ankylosis of the hip/knee may occur spontaneously, and it may be unnecessary to perform arthrodesis. Conversion of ankylosis or arthrodesis should be covered by antituberculosis treatment for 3 months before surgery and 9 months postoperatively. There is a low probability of reactivation if: >10 years since infection Solid arthrodesis Previous medical treatment. This is followed by a continuation phase with rifampicin and isoniazid, which is usually continued for a period of 69 months. It is now thought that extending chemotherapy beyond a year is required in only rare circumstances. The examiners were having none of this and more or less just concentrated on drug treatment of the disease. I must admit I did struggle a bit and the examiners would not let go of it and move on to something else. Subtrochanteric osteotomy and medial displacement of the femoral shaft with a tibial graft bridging the femur and ischium are carried out. It is a clever concept based on the principle that compression provided by the adduction forces will induce hypertrophy of the tibial graft (as opposed to iliofemoral grafts, which are under distraction). The structure that is particularly at risk when performing an ischiofemoral arthrodesis is the sciatic nerve.
Aqua Pimentae (Allspice). Detrol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96125
The radial nerve spirals medial to lateral posteriorly (13 cm from the trochlea) and then pierces the lateral intermuscular septum (7 medicine qhs proven 4 mg detrol. The ulnar nerve is medial to the brachial artery in the arm prior to piercing the medial intermuscular septum to pass posterior to the medial epicondyle. The median nerve crosses the brachial artery lateral to medial in the arm and enters the cubital fossa, which is formed by the distal humerus proximally, the pronator teres medially and the brachioradialis laterally. Access to olecranon fossae Posterolateral portal: access to radiocapitellar joint. Tendinopathies Repetitive tensile overload, which exceeds tissue stress tolerance, causes tissue damage. There is granulation-like tissue which consists of immature fibroblasts and disorganized non-functional vascular elements termed as angiofibroblastic hyperplasia. Detach intermuscular septum and reflect triceps posteriorly to expose the posterior joint. Arthroscopic portals Examination corner Basic science oral Identification of different bands of the medial and lateral collateral ligaments, function Identification of neurovascular bundles around the elbow Surgical approaches, internervous and intermuscular planes. This is frequently used as the initial entry portal to inflate the joint with saline Anterolateral portal: 1 cm distal and 1 cm anterior to the lateral epicondyle, between the radial head and the capitellum. This gives good access to the anterior aspect of the joint Anteromedial portal: 2 cm distal and 2 cm anterior to the medial epicondyle. Counterforce bracing reduces the force transmitted to the tendon origin/prevents full expansion of the muscle, therefore preventing maximal contraction. There are six key forearm exercises: wrist flexion/ extension, forearm supination/pronation and finger extension/ flexion with gradual increase in the resistance, repetitions and gradual decrease in forearm support during the exercises. Now show me the points of maximum tenderness for tennis elbow and the other conditions mimicking tennis elbow. Principles behind non-operative and operative treatments for tendinopathies Describe picture of elbow with depigmented skin with fat/skin atrophy may be a starting point! Provocative test Differential diagnosis Radiocapitellar degeneration (2 cm distal to the lateral epicondyle) and radial tunnel syndrome (4 cm distal to the lateral epicondyle). Tennis elbow will have a point of maximum tenderness just distal to the lateral epicondyle. Posterior tennis elbow this is degenerative tendinosis of the triceps tendon insertion. Surgically treatment is by debridement (not more than 50% tendon excision) and direct side-to-side repair. Tendon ruptures Distal biceps rupture A predisposing factor for rupture is degeneration in the hypovascular zone close to the radial tuberosity insertion. Mechanical irritation also plays a role there is 50% reduction in the interosseous space in pronation.
Proteins medical treatment 80ddb 4 mg detrol order with mastercard, oligonucleotides, and genes demonstrate poor oral bioavailability due to the harsh environment of the gastrointestinal tract and their relatively large size and rapid metabolism. The pulmonary route enables higher rates of passage in to systemic circulation than does oral administration. Factors influencing lung deposition are (1) physicochemical properties of the droplets or particles being delivered, (2) mechanical aspects of aerosol dispersion, and (3) the physiological and anatomical features of the lung. The particle size range should preferably be between 3 and 5 m if the inhaled drug is intended to penetrate to the small bronchioles and the lung alveoli and provide a rapid effect. Percutaneous absorption of a drug generally results from direct penetration of the drug through the stratum corneum, deeper epidermal tissues, and the dermis. Among the factors influencing percutaneous absorption are the physicochemical properties of the drug, including its molecular weight, solubility, partition coefficient, nature of vehicle, and condition of the skin. Chemical permeation enhancers, iontophoresis, or both are often used to enhance the percutaneous absorption of a drug. In general, patches are composed of three key compartments: a protective seal that forms the external surface and protects it from damage, a compartment that holds the medication itself and has an adhesive backing to hold the entire patch on the skin surface, and a release liner that protects the adhesive layer during storage and is removed just prior to application. Most patches belong to one of two general types-the reservoir system and the matrix system. Marketed transdermal patches are exemplified by Estraderm (estradiol), Testoderm (testosterone), Alora (estradiol), Androderm (testosterone), and Transderm-Scop (scopolamine). These devices are mostly used for contraception by preventing the fertilization of the egg by the sperm, inhibiting tubular transport, and/or preventing the implantation of the blastocyst in to the uterine endometrium. The hormone containing devices can be used for other hormonal effects such as in menorrhagia. The use of these devices can provide much lower systemic and high local progestogen levels. It is designed to provide an initial drug release rate of 20 g/day and is used to provide contraception for up to 5 years. What are the differences in the principle of drug delivery between an osmotic minipump and a diffusion controlled implant In Pharmacokinetics and Pharmacodynamics of Biotech Drugs: Principles and Case Studies in Drug Development, Meibohm B (ed. Describe the differences between the primary, secondary, and tertiary protein structures 2. Describe major pathways of protein degradation, their chemistry, and the corresponding stabilization strategies 4. More recently, an increasing number of pharmaceutical products comprise proteins and peptides.
Syndromes
Additional information:
Usage: q.d.
Tags: generic detrol 2 mg buy line, detrol 1 mg buy with amex, cheap 2 mg detrol with mastercard, discount detrol 4 mg buy line
Josh, 35 years: The blocking have a temporary effect but can reduce the inflammatory component that causes nerve irritation and pain - Neurolysis: the objective is to prevent the nerve send pain signals to the brain, for it, is injected alcohol or phenol around the nerve affected, in order to destroy and disrupt the nerve function. Experimental intervertebral disc degeneration; morphologic and proteoglycan changes over time. Ultimately she underwent a corrective osteotomy and posterior instrumented fusion.
Konrad, 41 years: Endometriosis and the appendix: a case series and comprehensive review of the literature. Atwal and colleagues examined hysterectomy specimens and found a significantly higher nerve fibers density in the endometrium of patients with pain symptomatology (whether with or without endometriosis) compared to patients without a painful disorder, independent from endometriosis (Atwal, et al. This manoeuvre stretches the piriformis muscle and elicits pain when the muscle is tight or involved with tendonitis.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





