
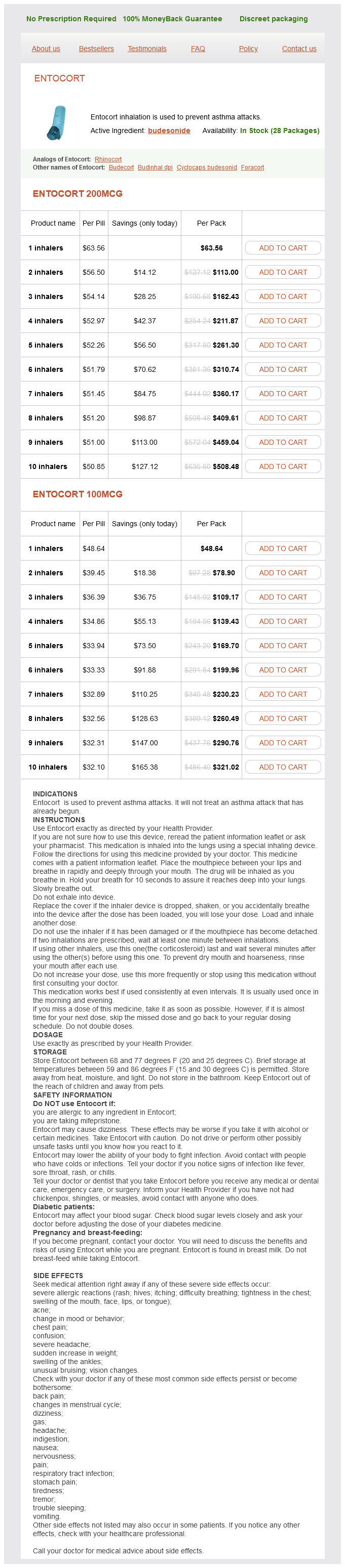
Entocort dosages: 200 mcg, 100 mcg
Entocort packs: 1 inhalers, 2 inhalers, 3 inhalers, 4 inhalers, 5 inhalers, 6 inhalers, 7 inhalers, 8 inhalers, 9 inhalers, 10 inhalers
In stock: 558
Only $34.11 per item
Reduction should be performed allergy testing kalispell mt cheap entocort 100 mcg visa, and pinning of the joints is required to ensure stability. Persistent hand weakness is common, and splinting combined with early therapy is recommended. Occasionally, dislocations of the metacarpophalangeal joints or the proximal interphalangeal joints are irreducible due to entrapment of the soft tissues and will require an open reduction. In particular, crush injuries, distal radius fracture, wrist dislocations and fracture dislocations, and burn injuries have a substantial rate of acute carpal tunnel syndrome. The carpal tunnel is a small fixed-volume space that physiologically acts like a closed space. With acute trauma to the forearm, wrist, and hand, pressure buildup can exceed inflow pressures of the epineural vessels. This leads to acute nerve ischemia, which manifests as tingling, burning pain, and numbness in the median nerve distribution. Loss of normal two-point discrimination (<6 mm) with readings greater than 15 mm indicates 100% sensory loss and, combined with history and overall examination, should establish the diagnosis. Carpal tunnel release performed within 40 hours of the onset of symptoms has been shown to hasten the recovery of normal nerve function. In the acute setting, closed reduction and splinting in a functional position can temporize most injuries. It is characterized by a complete loss of scapulothoracic articulation, typically with intact skin. Vascular and neurologic injuries are common, and when severe, the result is essentially a closed forequarter amputation. The literature on the topic consists mainly of case reports, small case series, and reviews. One of the largest reported series consists of 25 patients, treated over a 24-year period. Osseous and ligamentous injuries include clavicle fractures and acromioclavicular and sternoclavicular dislocations. Soft tissue destruction may involve the deltoid, latissimus dorsi, levator scapulae, pectoralis minor, rhomboid, and trapezius muscles. Vascular injuries to the subclavian or axillary vessels and complete or partial avulsion of the brachial plexus are very common and when severe result in a functional forequarter amputation. The diagnosis can be difficult, as patients often have severe associated injuries that impede the conduct of complete physical examination or distract the clinician from the involved extremity. Furthermore, intact skin and normal bony anatomy of the arm may be misleading as to the extent of the underlying injury. Vascular injuries may be evidenced by the "six Ps": (1) pain, (2) pallor, (3) pulselessness, (4) paresthesias, (5) paralysis, and (6) poikilothermia. However, owing to the extensive collateral vascular network around the shoulder, a patient may have subclavian artery occlusion and still have a pulse in the distal extremity with a normal brachial-brachial index.
L-75-1362B (Forskolin). Entocort.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96999
In contrast allergy medicine getting pregnant purchase entocort 200 mcg fast delivery, exogenous second hits include surgical interventions, blood product transfusions, and missed injuries. A loss of this balance can cause additional tissue injury from the immune response itself or leave the individual susceptible to infection and sepsis. As our understanding of the immune response following injury grows, our ability to monitor and effectively manage the traumatized, critically ill patient will hopefully result in improved outcomes. This "first hit" primes the immune system for an exaggerated and potentially lethal inflammatory reaction to a secondary, otherwise nonlethal, stimulus ("second hit"). Endogenous second hits include cardiovascular instability, respiratory distress, metabolic derangements, and ischemia/reperfusion injuries. Fry I nfection is the major threat to recovery among most trauma patients who survive the successful resuscitation and intervention of the initial 24 hours following severe injury. The infectious risk may occur from environmental contamination that attended the injury process, or from endogenous microflora of disrupted organ structures within the patient. Similarly, the trauma patient receives a large measure of care in the critical care unit with multiple invasive tubes and monitoring devices and each serves as a portal for microbial entry and potential life-threatening infection. From injury until recovery, the trauma patient is exposed to pathogens at the site of injury and everywhere "the hands of man" have been in the process of treatment. Not only are there abundant opportunities for infection, but the trauma patient sustains a remarkable compensatory suppression of immune responses. Virtually every measurable component of the innate and adaptive immune response is suppressed. The exact benefit for the suppressed host is often hard to rationalize from an evolutionary perspective, but modulation of the wholesale systemic activation of the innate inflammatory response that is activated by major tissue injury must provide some protection for the injured host. However, the millennia of evolution did not anticipate aggressive resuscitation, surgical interventions, and critical care units. The contemporary end result is survival through incredible multisystem injury, only to have a recovering host that is a human Petri dish. This overview will briefly discuss a model of common clinical issues that cause infection in the care of trauma patients. This will not be a detailed discussion of each anatomic site of infection or a detailed discussion of pathogens and antibiotic choices because most are discussed in detail in other chapters. It will highlight the common features that are associated with the important infections of the trauma patient, and will use examples of specific infections and specific pathogens to emphasize these features. This overview will hopefully give a perspective to the many areas that deserve continued attention and investigation. All injured sites, all surgical incisions, and all invasive medical devices will have recoverable bacteria when cultured.
An abdominal radiograph should always be obtained to confirm appropriate position of the tube prior to initiating feedings allergy medicine is not working entocort 100 mcg cheap. With some modifications, this technique can also be used for postpyloric feeding tube placement. Second, the tube is advanced a bit further along the greater curvature of the stomach, until a point of resistance is met at the pylorus. Third, gentle pressure is maintained on the tube until the pylorus opens and the tube advances into the duodenum, and an abdominal radiograph is obtained to confirm the position of the tube in the duodenum. If long-term gastrointestinal access is indicated, a more invasive approach will be required. If special precautions are taken, this procedure can also be performed safely in patients with a history of previous abdominal surgery. Above all, it is important to know if any gastrointestinal anatomic changes have resulted from the previous surgery. It is important to obtain abdominal films and review prior scans to be certain that the stomach is approachable through a safe abdominal wall window. During endoscopy, a bright light should be seen transabdominally in an area accessible for tube placement. A finder needle should be inserted through the abdominal wall into the stomach to ensure that as air is aspirated into the syringe, the needle is visualized endoscopically in the lumen of the stomach. These antimicrobial catheters may be placed into patients either temporarily at the bedside or permanently in an operative suite. In addition, the catheters may be placed by accessing a central vein directly or indirectly by using a peripheral venous access route. The routine use of venous Doppler devices has been demonstrated to decrease complications related to venipuncture. These catheters may be made of silicone or polyurethane and are available with single or double lumens in gauges from 16 to 23. A flexible stylet or guidewire is provided in the commercially available kit to help with insertion using a Seldinger technique with a peel-away sheath or by using a catheter-over-the-needle technique. Combination tubes are available having an inner jejunostomy portion of the gastrostomy tube that can be placed transpylorically. These tubes can also be placed in the radiology suite by a specially trained interventional radiology team. It is important to remember that tubes placed transabdominally, under fluoroscopic guidance alone, puncture and enter the stomach, but are not secured to the abdominal wall as with the open techniques.
Syndromes
Additional information:
Usage: p.c.
Tags: entocort 200 mcg buy without a prescription, purchase entocort 200 mcg mastercard, entocort 200 mcg purchase, discount 100 mcg entocort with mastercard
Cole, 50 years: Among survivors at 24 hours, the subsequent risk of death by day 30 was not associated with plasma or platelet ratios.
Tuwas, 59 years: Of note, the use of fibrinolytics does not increase survival in patients with ongoing cardiogenic shock.
Darmok, 53 years: Based on these and other similar study results, many groups targeted resuscitation of severely injured trauma patients to achieve physiologic values retrospectively associated with survival.
Rathgar, 51 years: Posterior teardrop fractures usually occur from a flexion-compression mechanism, often involve all three columns of the spinal canal, and often involve neurologic compromise.
Shakyor, 65 years: Regular use of oral care with chlorhexidine in mechanically ventilated patients has been associated with which of the following
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





