
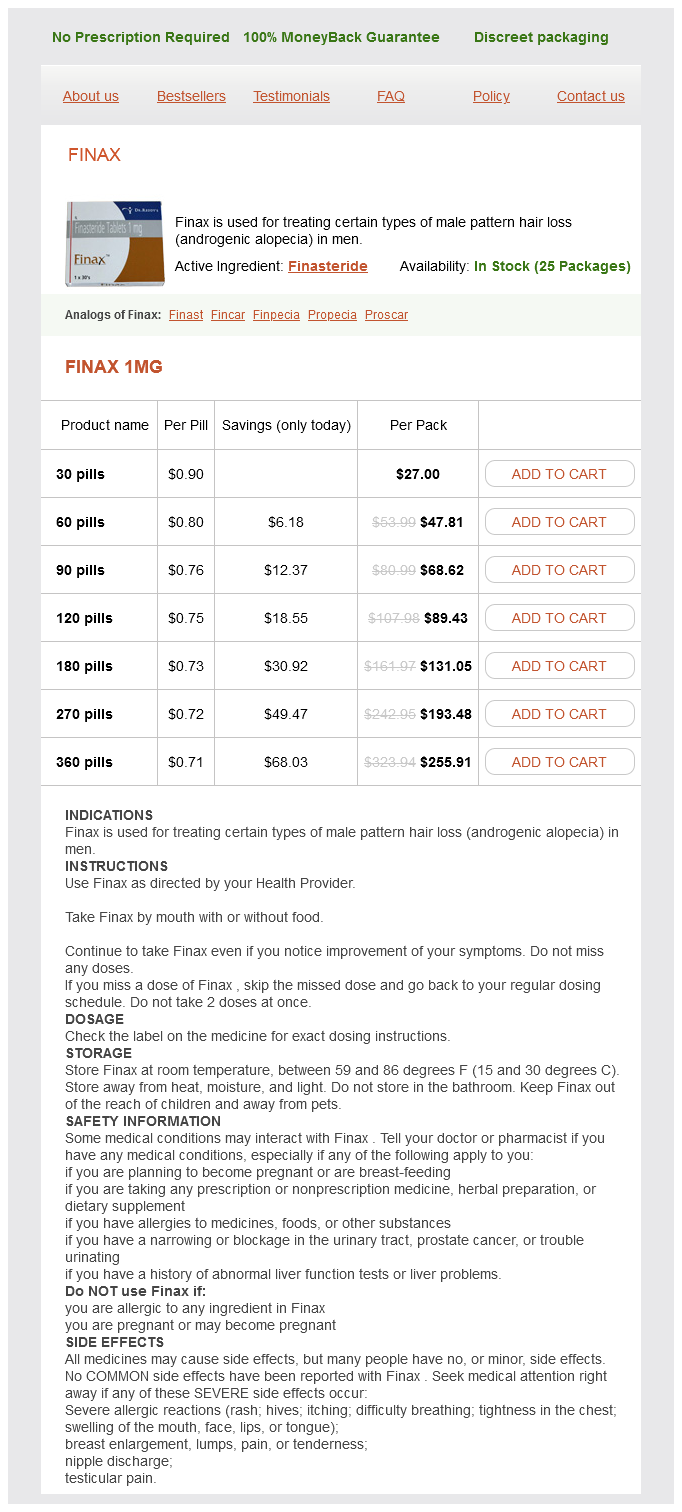
Finax dosages: 1 mg
Finax packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 674
Only $0.76 per item
Pubococcygeus muscle · Weakening and opening of the urogenital hiatus from neuromuscular injury to the pelvic floor muscles is thought to contribute to urogenital prolapse as described later in the chapter symptoms 7dp3dt generic finax 1 mg without a prescription. Ligaments Key Point · the round and broad ligaments of the uterus consist of smooth muscle and loose areolar tissue, respectively, and do not contribute to the support of the uterus and adnexa. In contrast, the cardinal and uterosacral ligaments do contribute to pelvic organ support. The round and broad "ligaments" of the uterus consist of smooth muscle and loose areolar tissue, respectively, and do not contribute to the support of the uterus and adnexae. In contrast, the cardinal and uterosacral "ligaments" do contribute to the support of the uterus and upper third of the vagina. The cardinal ligaments primarily consist of perivesical connective tissue and nerves and are vertically oriented in the anatomic or standing position. The uterosacral ligaments consist primarily of smooth muscle and contain some of the pelvic autonomic nerves. In the anatomic position, the uterosacral ligaments are directed posteriorly and oriented almost horizontal to the floor. Although the term ligament is most often used to describe dense connective tissue that connects two bones, the "ligaments" of the pelvis are variable in composition, site of attachments, and function. The pelvic ligaments range from connective tissue structures that support the bony pelvis and pelvic organs to smooth muscle and loose areolar tissue that add no significant support. The sacrospinous, sacrotuberous, and anterior longitudinal ligament of the sacrum consist of dense connective tissue that join bony Clinical Correlations · the sacrospinous and anterior longitudinal ligament serve as suture fixation sites in suspensory procedures used to correct pelvic organ prolapse. It exits the pelvis through the lesser sciatic foramen, attaches to the greater trochanter of the femur, and as the piriformis muscles, it functions as an external hip rotator. Pelvic parietal fascia provides muscle attachment to the bony pelvis and serves as anchoring points for visceral fascia, also termed endopelvic fascia, which will be described later in the chapter. Condensations or thickening of the parietal fascia covering the medial surface of the obturator internus and levator ani muscles serve special functions. The arcus tendineus levator ani is a condensation of fascia covering the medial surface of the obturator internus muscle. This structure serves as the point of origin for parts of the very important levator ani muscles. The arcus tendineus fascia pelvis is a condensation of fascia covering the medial aspect of the obturator internus and levator ani muscles. It represents the lateral point of attachment for the distal portion of the anterior vaginal wall. The proximal portion of the arcus tendineus fascia pelvis also contributes to the lateral point of attachment for the iliococcygeal muscles. The levator ani muscles represent the main muscular component of the pelvic floor and are discussed later in the chapter. Piriformis Muscle this muscle arises from the anterior and lateral surface of the sacrum and partially fills the posterolateral pelvic walls.
Monarda didyma (Oswego Tea). Finax.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96206
This passive fixation stabilizes the urethrovesical junction and enables increases in abdominal pressure to be transmitted to the proximal urethra and bladder neck during times of stress medications used to treat schizophrenia generic finax 1 mg with amex, such as coughing, sneezing, laughing, or running. The Burch colposuspension is generally performed through a Pfannenstiel or Cherney incision and if performed without a concomitant intra-abdominal procedure, one can remain preperitoneal obviating the need for bowel packing. In order to avoid the potential complications associated with laparotomy, in the 1990s, endoscopic surgeons began to perform Burch procedures via the laparoscope. In skilled hands, reported cure rates were comparable to those obtained with the open procedure. Patients tended to have fewer associated perioperative complications, less postoperative pain, and decreased hospital stay as compared with open colposuspension, but operative time was longer and associated costs were higher. Abdominal and/or vaginal repairs for correction of prolapse are often performed concomitantly with a Burch colposuspension. At the preoperation urodynamic evaluation, it is important to perform provocative leak point determinations with the prolapse both reduced with a ring forceps and in the unreduced state. The kinking of the urethra with a prolapsed bladder can mask stress incontinence that may become apparent in the postoperative period after correction of the prolapse. Consent As in all surgeries where a laparotomy is performed, there is the potential for blood loss, wound infection, and delayed return of bowel function if the peritoneal cavity is entered. The Burch procedure itself can present intraoperative complications including urethral or bladder injury, ureteral injury, and bleeding in the retropubic space. Even in the hands of experienced surgeons, the Burch colposuspension can be challenging in obese patients, with large amounts of fat in the retropubic space, or patients with a stenotic vaginal canal. Postoperative voiding dysfunction, particularly de novo urinary urgency, and the formation of enterocele due to the anterior deflection of the anterior vaginal wall have been reported. Antibiotic Prophylaxis Antibiotic prophylaxis, administered preoperatively, is warranted before performance of a Burch colposuspension. A first-generation cephalosporin such as cefazolin, 1 g intravenously, given before surgery is generally sufficient. Intraoperative Anesthesia and Patient Positioning After induction of general or regional (spinal or epidural) anesthesia, the patient is placed in dorsal lithotomy position using Allen stirrups taking care not to overextend or flex the legs with the weight of the leg on the heel of the foot (Allen Medical Systems, Acton, Massachusetts). The abdomen and vagina are surgically prepped and a 16Fr or 18Fr Foley catheter is placed in the bladder connected to closed drainage. Abdominal Incision A Pfannenstiel or Cherney incision is made approximately 1 cm above the upper margin of the pubic symphysis. A low rectus fascial incision is preferred to allow easier access to the retropubic space. If a hysterectomy, adnexectomy, or other intraperitoneal procedure is planned, careful undermining of the rectus muscles off the underlying peritoneum into the retropubic space is performed prior to entering the abdominal cavity in order to facilitate further dissection after the intra-abdominal procedure is completed.
Given that the immunophenotypic features overlap with many of the aforementioned tumors symptoms 16 weeks pregnant 1 mg finax order amex, a panel of immunostains is generally required. As mentioned previously, a combination of immunohistochemical and molecular assays should allow for these distinctions. The tumor mainly affects young adults; its principal sites are the fingers, hands, and forearms. Clinical Findings Epithelioid sarcoma is most prevalent in adolescents and young adults 10 to 35 years of age, with a median age in the mid-20s. Male patients outnumber females by about 2 to 1,478-482 and there is no ethnic (race) predilection. The tumor most often arises on the flexor surfaces of the fingers, hands, and forearm, followed by the knee and lower leg, especially the pretibial region, the buttocks and thigh, the shoulder and arm, and the ankle, foot, and toe. It is rare in the trunk and head and neck region, with the exception of the scalp. When located superficially, it usually presents as a firm nodule that may be solitary or multiple, has a calluslike consistency, and is often described as a woody hard knot or firm lump that is slowly growing and painless. Nodules situated in the dermis are often elevated above the skin surface and frequently become ulcerated weeks or months after they are first noted. Pain or tenderness is rarely a prominent symptom, with the exception of the tumors that encroach on large nerves. In a 1998 follow-up study, 25 of 35 patients with available follow-up died of widespread metastasis, and the remainder were alive with disease. Radiographic examination typically reveals a soft tissue mass with an occasional speckled pattern of calcification. Cortical thinning and erosion of underlying bone may be present, but invasion and destruction of adjacent bone are rare. Deepseated tumors, attached to tendons or fascia, tend to be larger and present as firm, multinodular masses with irregular outlines. The cut surface has a glistening, gray-white or gray-tan, mottled surface with focal yellow or brown areas caused by focal necrosis or hemorrhage. Proximaltype epithelioid sarcoma tends to be larger and more infiltrative than the distal type. Because many lesions are multinodular, determination of their exact size is often impossible. Histologically, the conventional (classic) type of epithelioid sarcoma has a distinct nodular arrangement of the tumor cells, a tendency to undergo central degeneration and necrosis, and an epithelioid appearance with cytoplasmic eosinophilia. The nodular pattern, probably the most conspicuous single feature of this tumor, varies somewhat. Multiple nodules are less common in tissue obtained at the initial operation than in recurrent tumors. In rare cases the presence of multiple small, superficial satellite nodules near the operative site may mimic a dermatologic disease. When the tumor spreads within a fascia or aponeurosis, it forms festoonlike or garlandlike bands punctuated by areas of necrosis.
Syndromes
Additional information:
Usage: q.d.
Tags: 1 mg finax purchase with mastercard, generic finax 1 mg on line, purchase 1 mg finax visa, cheap finax 1 mg without a prescription
Fedor, 48 years: During genital arousal, the proximal vagina distends and the vessels of the vaginal subepithelium become engorged, allowing a transudative fluid to diffuse across the vaginal epithelium. Injuries to inferior parts of the brachial plexus (Klumpke paralysis) are much less common. At the sites of anastomoses between portal and systemic veins, portal hypertension produces enlarged varicose veins and blood flow from the portal to the systemic system of veins. Avascular necrosis of the proximal fragment of the scaphoid (pathological death of bone resulting from poor blood supply) may occur and produce degenerative joint disease of the wrist.
Aschnu, 49 years: In modern preoperative counseling regarding alternatives for surgery, Need for Continence Surgery with Prolapse Surgery If surgery for stress incontinence is indicated at the same time as prolapse surgery, either the abdominal or vaginal route may be employed. In infundibular pulmonary stenosis, the conus arteriosus is underdeveloped, producing a restriction of right ventricular outflow. With the widespread use of synthetic polypropylene mesh for the treatment of stress urinary incontinence and/or pelvic organ prolapse, mesh exposures and mesh contractures may occur and have been associated with dyspareunia. Other ways to compensate are to lift the foot higher as it is brought forward or to swing the foot outward.
Shakyor, 46 years: B, Higher-power view shows cell nests that are separated by thin-walled, sinusoidal vascular spaces. Historically this has most often been accomplished through the use of biofeedback. In fact, one can see different growth patterns in different areas of the same tumor. The levels of the kidneys change during respiration and with changes in posture of Median plane Scapular line Diaphragm Liver Spleen T10 T11 Transpyloric plane Left kidney 12th rib Right kidney Ureter Iliac crest Ilium Dimple indicating posterior superior iliac spine (A) Posterior view L4 L5 T12 L1 5cm 23 cm in a vertical direction.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





