
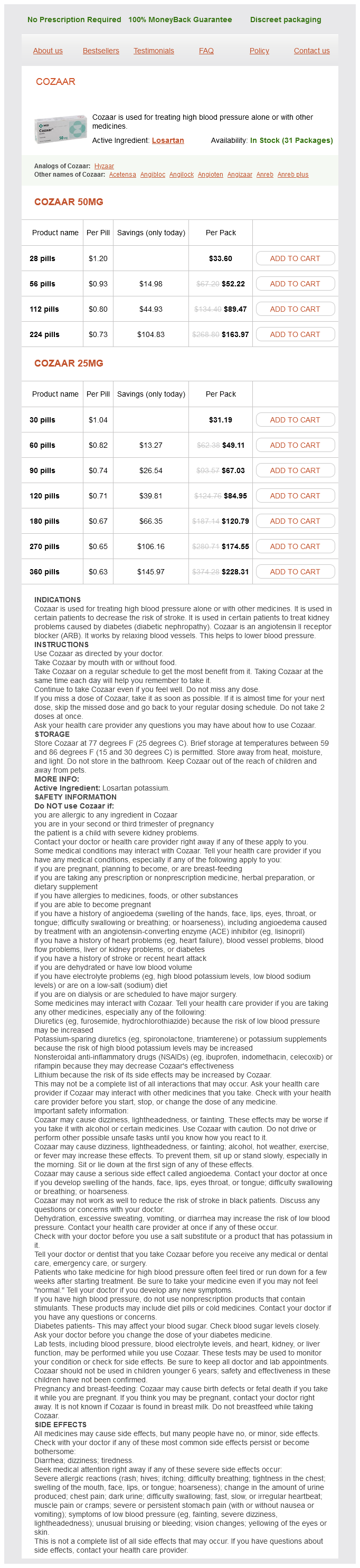
Losartan dosages: 50 mg, 25 mg
Losartan packs: 28 pills, 56 pills, 112 pills, 224 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 715
Only $0.67 per item
To drain convexity subdural collection to reduce increased intracranial pressure or to prevent the development of craniocerebral disproportion Repeated therapeutic subdural taps should not be performed unless the infant is symptomatic or the head size is growing rapidly diabetes x cerveja 50 mg losartan purchase overnight delivery. Surgical intervention is indicated if subdural taps are not effective in controlling these symptoms (2). Insert the needle as far laterally as possible at the border of the anterior fontanelle or along the coronal suture, at least 1 to 2 cm from the midline, to avoid puncturing the sagittal sinus. Remove the needle if there is not a definite change in resistance on penetrating the dura after insertion to approximately 0. Hold the needle securely at all times to avoid inadvertent movement of the needle tip. Grasp the needle firmly or apply a hemostat at approximately 1 cm from the beveled end of the needle, to prevent inadvertent advancement of the needle into the cerebral cortex. If frequent taps are required, vary the puncture site slightly to prevent fistula formation. Following the procedure, apply pressure to the scalp for 2 to 3 minutes to prevent fluid leak from the puncture site or subgaleal fluid collection. Gloves and face mask Cup with iodophor antiseptic solution Gauze swabs Drapes or surgical towels Two short bevel needles, 19 to 22 gauge × 1 inch, with stylets 6. Locate the coronal suture by palpation at the lateral corner of the anterior fontanelle. Generally, anesthesia is not required, but local injection of lidocaine at this time or application of topical anesthetic cream prior to cleaning the area can be used for local anesthesia at the puncture site (1,1013). Insert the needle slowly through the coronal suture, just lateral to its junction with the anterior fontanelle. As the needle advances through the skin, pull the scalp slightly to create a Z-like track through the underlying tissue. This will help prevent fluid leakage from the puncture site or into the subgaleal space after removal of the needle. Allow fluid to drain spontaneously into the sterile tubes until flow ceases or a maximum volume of 15 to 20 mL. After removing the needle, apply firm pressure to the puncture site with sterile gauze for 2 to 3 minutes. Coronal section of anatomic drawing showing subdural needle penetrating the dura in a patient with bilateral convexity subdural fluid collections. Subdural bleeding from laceration of the superior sagittal sinus or smaller vessels or from removal of excessive fluid with shift of intracranial contents and rebleeding 2. Development of chronic subdural fluid collection (14,15) this complication may develop more frequently in infants treated with subdural tap. Infection In one small case series, 1 of 12 infants (8%) treated with subdural tap developed subdural empyema after multiple taps (15). Intracranial hemorrhage: subdural, primary subarachnoid, intracerebellar, intraventricular (term infant), and miscellaneous. A critical review of the topical local anesthetic amethocaine (Ametop) for pediatric pain.
Hagenia abyssinica (Kousso). Losartan.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96886
Lange F (1910) Support for the spondylitic spine by means of buried steel bars blood sugar drop order 50 mg losartan overnight delivery, attached to the vertebrae. Magerl F (1982) External skeletal fixation of the lower thoracic and upper lumbar spine: current concepts of external fixation of fractures. Medical Research Council (1978) Five-year assessments of controlled trials of ambulatory treatment, debridement and anterior spinal fusion in the management of tuberculosis of the spine. Mukopadhahya B (1958) the role of excisional surgery in the treatment of bone and joint tuberculosis. Paulus of Aegina (1844 1847) Seven Books of Paulus of Aegina translated by Adams F. Pott P (1779) Remarks on that kind of the lower limbs, which is frequently found to accompany a curvature of the spine, and is supposed to be caused by it. Roy-Camille R, Roy-Camille M, Demeulenaere C (1970) Osteosynthesis of dorsal, lumbar, and lumbosacral spine with metallic plates screwed into vertebral pedicles and articular apophyses, Presse Med 78:1447 1448 102. Travers B (1824) Curious case of anchylosis of great part of the vertebral column, probably produced by an ossification of the intervertebral substance. Histoire et m´moires de la Soci´t´ des sciences physiques de Lausanne, 1: 66, 2: e ee 197 207 (separate edition by Lausanne: J. Verbiest H (1954) A radicular syndrome from development narrowing of the lumbar vertebral canal. Verbiest H (1955) Further experiences on the pathological influence of a developmental narrowness of the bony lumbar vertebral canal. Vesalius A (1543) De Humani Corporis Fabrica Liberi Septum, Basel: Ex officina Ionnis Oporini 117. Clin Orthop 117:23 Chapter 1 37 Basic Science Section 41 Biomechanics of the Spine 2 Core Messages Stephen Ferguson the main functions of the spine are to protect the spinal cord, to provide mobility to the trunk and to transfer loads from the head and trunk to the pelvis the trabecular bone bears the majority of the vertical compressive loads the vertebral endplate plays an important role in mechanical load transfer and the transport of nutrients Axial disc loads are borne by hydrostatic pressurization of the nucleus pulposus, resisted by circumferential stresses in the anulus fibrosus Approximately 10 20 % of the total fluid volume of the disc is exchanged daily Combined axial compression, flexion and lateral bending have been shown to cause disc prolapse the facet joints guide and limit intersegmental motion the ligaments surrounding the spine guide segmental motion and contribute to the intrinsic stability of the spine by limiting excessive motion the spatial distribution of muscles determines their function. Changes to segmental laxity ("neutral zone") are associated with trauma and degeneration the highest loads on the spine are produced during lifting the Human Spine the human spinal column is a complex structure composed of 24 individual vertebrae plus the sacrum. The principal functions of the spine are to protect the spinal cord, to provide mobility to the trunk and to transfer loads from the head and trunk to the pelvis. By nature of a natural sagittal curvature and the relatively flexible intervertebral discs interposed between semi-rigid vertebrae, the spinal column is a compliant structure which can filter out shock and vibrations before they reach the brain. The intrinsic, passive stability of the spine is provided by the discs and surrounding ligamentous structures, and supplemented by the actions of the spinal muscles. The seven intervertebral ligaments which span each pair of adjacent vertebrae and the two synovial joints on each vertebra (facets or zygapophyseal joints) allow controlled, fully three-dimensional motion. The spine can be divided into four distinct regions: cervical, thoracic, lumbar and sacral. The cervical and lumbar spine are of greatest interest clinically, due to the substantial loading and mobility of these regions and associated high incidence of trauma and degeneration. The thoracic spine forms an integral part of the ribcage and is much less mobile due to the inherent stiffness of this structure.
Several events may precipitate acute gouty arthritis: dietary excess diabetes type 2 early warning signs buy generic losartan 25 mg, trauma, surgery, excessive ethanol ingestion, hypouricemic therapy, and serious medical illnesses such as myocardial in arction and stroke. A er many acute mono- or oligoarticular attacks, a proportion o gouty patients may present with a chronic nonsymmetric synovitis, causing potential con usion with rheumatoid arthritis (Chap. Most women with gouty arthritis are postmenopausal and elderly, have osteoarthritis and arterial hypertension that causes mild renal insuf ciency, and usually are receiving diuretics. Kindreds o precocious gout in young emales caused by decreased renal urate clearance and renal insuf ciency have been described. Acute septic arthritis, several o the other crystalline-associated arthropathies, palindromic rheumatism, and psoriatic arthritis may present with similar clinical eatures. Bacterial in ection can coexist with urate crystals in synovial uid; i there is any suspicion o septic arthritis, joint uid must be cultured. Arthrocentesis o these joints is a use ul technique to establish the diagnosis o gout between attacks. Serum uric acid levels can be normal or low at the time o an acute attack, as in ammatory cytokines can be uricosuric and e ective initiation o hypouricemic therapy can precipitate attacks. Nevertheless, serum urate levels are almost always elevated at some time and are important to use to ollow the course o hypouricemic therapy. A 24-h urine collection or uric acid can, in some cases, be use ul in assessing the risk o stones, elucidating overproduction or underexcretion o uric acid, and deciding whether it may be appropriate to use a uricosuric therapy. Excretion o >800 mg o uric acid per 24 h on a regular diet suggests that causes o overproduction o purine should be considered. Ultrasound may aid earlier diagnosis by showing a double contour sign overlying the articular cartilage. Dual-energy computed tomography (C) can show speci c eatures establishing the presence o urate crystals. These crystals are strongly nega tive bire ringent crystals under compensated polarized light microscopy; 400×. The drug must be at least temporarily discontinued promptly at the rst sign o loose stools, and symptomatic treatment must be given or the diarrhea. Hypouricemic drug therapy should be considered when, as in most patients, the hyperuricemia cannot be corrected by simple means (control o body weight, lowpurine diet, increase in liquid intake, limitation o ethanol use, decreased use o ructose-containing oods and beverages, and avoidance o diuretics). The decision to initiate hypouricemic therapy usually is made taking into consideration the number o acute attacks (urate lowering may be cost-e ective a er two attacks), serum uric acid levels (progression is more rapid in patients with serum uric acid >535 µmol/L [>9. Uratelowering therapy should be initiated in any patient who already has tophi or chronic gouty arthritis.
Syndromes
Additional information:
Usage: p.c.
Tags: purchase losartan 25 mg with visa, buy 50 mg losartan visa, losartan 50 mg without prescription, cheap 50 mg losartan with mastercard
Mason, 52 years: In ammatory arthritis is likely i there is prolonged morning sti ness and many other joints are a ected.
Ilja, 28 years: Pulse oximetry can be used reliably in very low-birthweight infants with acute as well as chronic lung disease (911).
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





