
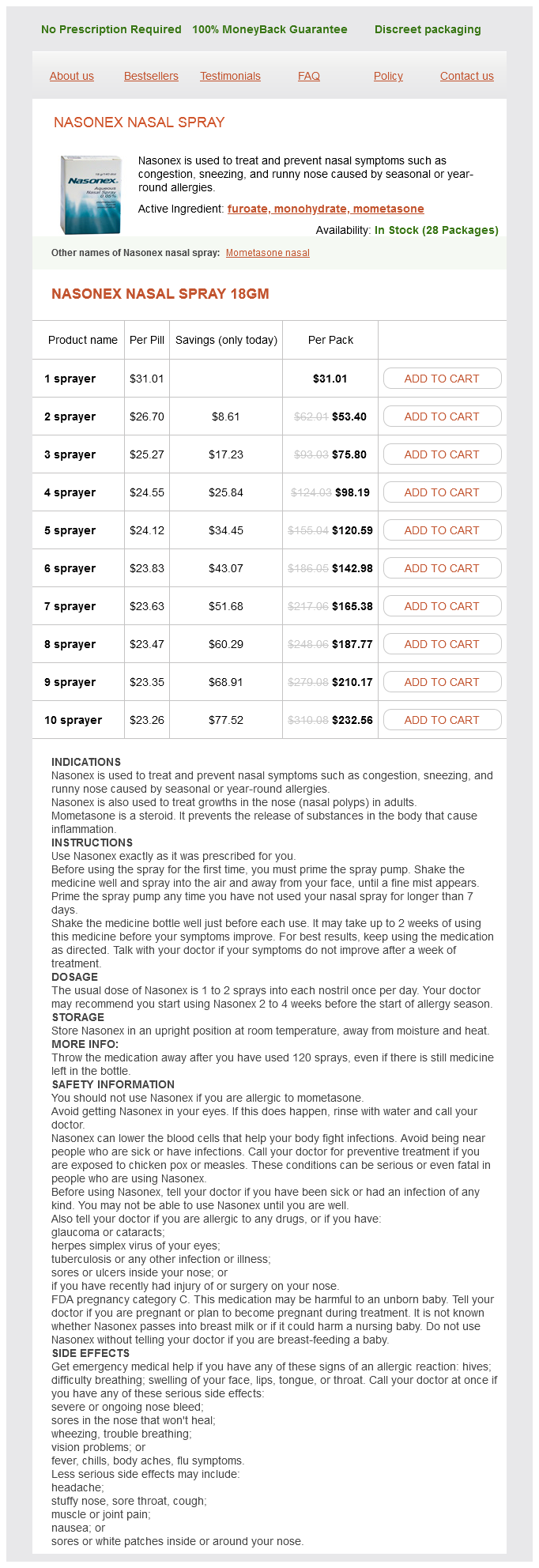
Nasonex nasal spray dosages: 18 gm
Nasonex nasal spray packs: 1 sprayer, 2 sprayer, 3 sprayer, 4 sprayer, 5 sprayer, 6 sprayer, 7 sprayer, 8 sprayer, 9 sprayer, 10 sprayer
In stock: 829
Only $24.71 per item
The GuardWire system is much less steerable than con ventional coronary guidewires allergy shots while breastfeeding buy nasonex nasal spray 18 gm otc. The system must be advanced across the target lesion and positioned at least 20 mm dis tally. The stent/angioplasty balloon is loaded over the wire and positioned proximal to the lesion, and the GuardWire balloon is inflated. A small contrast inj ection allows visualiza tion up to the occlusive balloon and confirms interruption of antegrade flow. All embolic material is trapped in the stagnant column of blood proximal to the balloon and aspirated with the Export catheter before the GuardWire balloon is deflated and antegrade flow is restored. Extreme attention must be paid to avoiding kinking of the hypo tube resulting in failure of the balloon to deflate. Should this happen if ever, the hypotube should be cut distal to its gold marker to allow deflation. Filters also have the po tential to traumatize the distal vessel, and advancement of filter retrieval sheaths through freshly deployed stents is sometimes difficult. I t consists of a conven tional guidewire to which an elliptical, radiopaque, nitinol loop is attached. A polyurethane filter bag with 1 1 0-micron pores is suspended from the nitinol loop. Distal Filters Filtration devices utilize a nonocclusive basket deployed dis tal to the target lesion to capture embolic material larger than the interstices of the device mesh. Advantages: Preserved antegrade coronary flow is a dis tinct advantage of the filter approach, minimizing ischemia and allowing angiographic visualization of the target lesion and distal vasculature during the period of embolic protec tion. The delivery and retrieval steps are intuitive to most interventionalists, often employing standard coronary guide wires to cross the lesion rather than a less responsive, bulkier occlusion balloon-wire apparatus. The requisite need to traverse the target lesion incurs some risk of device-induced distal embolization before protection is established. The completeness of distal protection may also be compromised when the filter is positioned in tortuous segments where apposition of the basket against the vessel wall is suboptimal. Smaller particulate matter and soluble factors still traverse the filter and enter the microcirculation. This requires either prompt use of an aspiration catheter to clear the filter or urgent filter retrieval to restore antegrade flow. In addi tion, filters require a distal landing zone of approximately 1 8 to 30 mm from a graft anastomosis in order to accom modate the length of the device, thereby limiting use of dis tal filtration in the setting of very distal lesions. The wire is designed to rotate and move longitudi nally independent of the filter for enhanced stability during the pro cedure. Submerged in saline to avoid air trapping, the wire is pulled into the tip of the catheter and back to a clear space in the catheter proximal to the coro nary guidewire monorail exit.
Jiang (Ginger). Nasonex nasal spray.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96924
During the early portion of the action potential allergy treatment for humans 18 gm nasonex nasal spray purchase, the ratio of sodium to potassium conductance increases more than 1000-fold. Therefore, far more sodium ions flow to the interior of the fiber than potassium ions to the exterior. This is what causes the membrane potential to become positive at the action potential onset. Then, the sodium channels begin to close, and the potassium channels begin to open; thus, the ratio of conductance shifts far in favor of high potassium conductance but low sodium conductance. This shift allows for a very rapid loss of potassium ions to the exterior but virtually zero flow of sodium ions to the interior. Roles of Other Ions During the Action Potential Thus far, we have considered only the roles of sodium and potassium ions in generating the action potential. At least two other types of ions must be considered, negative anions and calcium ions. Sodium conductance increases several thousandfold during the early stages of the action potential, whereas potassium conductance increases only about 30-fold during the latter stages of the action potential and for a short period thereafter. They include the anions of protein molecules and of many organic phosphate compounds and sulfate compounds, among others. Because these ions cannot leave the interior of the axon, any deficit of positive ions inside the membrane leaves an excess of these impermeant negative anions. Therefore, these impermeant negative ions are responsible for the negative charge inside the fiber when there is a net deficit of positively charged potassium ions and other positive ions. The membranes of almost all cells of the body have a calcium pump similar to the sodium pump, and calcium serves along with (or instead of) sodium in some cells to cause most of the action potential. Like the sodium pump, the calcium pump transports calcium ions from the interior to the exterior of the cell membrane (or into the endoplasmic reticulum of the cell), creating a calcium ion gradient of about 10,000-fold. This process leaves an internal cell concentration of calcium ions of about 10-7 molar, in contrast to an external concentration of about 10-3 molar. Because the calcium ion concentration is more than 10,000 times greater in the extracellular fluid than in the intracellular fluid, there is a tremendous diffusion gradient and elec- 70 Conductance (mmho/cm2) Chapter 5 trochemical driving force for the passive flow of calcium ions into the cells. These channels are slightly permeable to sodium ions and calcium ions, but their permeability to calcium is about 1000-fold greater than to sodium under normal physiological conditions. When the channels open in response to a stimulus that depolarizes the cell membrane, calcium ions flow to the interior of the cell. A major function of the voltage-gated calcium ion channels is to contribute to the depolarizing phase on the action potential in some cells. The gating of calcium channels, however, is relatively slow, requiring 10 to 20 times as long for activation as for the sodium channels. For this reason, they are often called slow channels, in contrast to the sodium channels, which are called fast channels. Therefore, the opening of calcium channels provides a more sustained depolarization, whereas the sodium channels play a key role in initiating action potentials. In fact, in some types of smooth muscle, the fast sodium channels are hardly present; therefore, the action potentials are caused almost entirely by the activation of slow calcium channels.
It is an asymmetric device to account Chaj>ter 35 Intervention for Pediatric and Adult Cong enital Heart Disease 852 for the surrounding cardiac structures allergy forecast frisco tx order nasonex nasal spray 18 gm free shipping. Older patients with larger defects, who have not been repaired, will most often have developed pulmonary vascular disease. Only the older patients, with adult onset symptoms are an ideal population for a transcatheter approach. The need for successful transcatheter therapy has therefore been more acute in patients with muscular rather than with the membranous defects. At the same time, the anatomy is more favorable to a transcatheter approach as most have good surrounding tissue rims to support the device, with out concerns of valvar or electrophysiologic compromise. With subsequent growth of the child, transcatheter defect closure would become technically easier and could be followed with surgical band removal (also a closed heart procedure). The defect is then crossed from the left ventricular septal surface, either with a torquable coronary catheter or with a balloon-tipped catheter (balloon wedge catheter) introduced retrograde via the femoral artery or ante grade via a transvenous transseptal approach. This creates a reliable "rail" over which the device delivery sheath can be passed. The wire is then removed from the arterial side and the device is delivered through the long sheath in the usual fashion. When angiographic and/or echo images confirm the position of the device on both sides of the septum, the device is released. For patients with membranous-type defects suffi ciently large to cause clinical symptoms, the surgical option remains an excellent alternative. In an era of aggres sive angioplasty at the first signs of ischemia, this compli cation of myocardial infarction is far less common than in previous generations. Untreated, large defects are nearly always fatal, as a large left-to-right shunt, pulmonary overcirculation, pulmo nary hypertension, and left ventricular volume overload are superimposed on a severely compromised/ischemic pump. Acute surgical intervention with patch closure has been dif ficult, because the surgeon has little reliable tissue in the margins of the defect in which to place sutures. Exclusion strategies similar to those used for apical aneurysms are now being more commonly employed. Similarly, following early transcatheter closure of large defects, ongoing necrosis of surrounding tissue can lead to important residual shunts and device instability after early implantation. Small defects are interesting from a diagnostic perspective, but do not impose a significant hemodynamic burden. Interestingly, though, with ongoing tissue necrosis, the defect can become more hemo dynamically important over the first few weeks. It is current teaching that these defects, once identified as hemodynamically important, should be closed as soon as pos sible, whether by a surgical or transcatheter approach. Wait ing for days to stabilize the patient medically is unreliable, as the shunt may only increase with time and the onset of multi system organ failure over several days of poor cardiac output makes the patient less likely to recover from either interven tion.
Syndromes
Additional information:
Usage: q.d.
Tags: generic nasonex nasal spray 18 gm mastercard, purchase nasonex nasal spray 18 gm fast delivery, nasonex nasal spray 18 gm buy without prescription, 18 gm nasonex nasal spray order free shipping
Georg, 58 years: Cerebral injury and neurodevelopmental impairment after amnioreduction versus laser surgery for twin-twin transfusion syndrome: a systematic review and meta-analysis. Outpatient coronary angiography for low- to moderate-risk patients began in the 1990s23. Diastolic Relaxation of the Heart: Basic Research and Soc Echocardiogr 2003; 1 6: 724-73 1. Pullback 2, identified that the systolic gradient was located within the ventricular chamber, at the subvalvar level.
Tangach, 46 years: In some patients, the differences in gradient among the different measurement sites were as much as 45 mmHg. Evaluation of biopsy clas sification for rejection: relation to detection of myocardial damage by monoclonal antimyosin antibody imaging. However, studies under saline or blood disclosed less efficient plaque abla tion and more intense photoacoustic effects. Middle aortic syn reveals a smooth tapered proximal and midabdominal aorta which include Williams syndrome, 123 neurofibromatosis, 124 congenital rubella,125 and tuberous sclerosis, 1 26 may also innominate artery), the left common carotid and left subcla vian arteries usually originate separately from the aortic arch.
Grok, 57 years: Obj ective measures of exercise capacity have cor roborated these clinical observations, though in uncontrolled 40 trials. Transcatheter fenestration dilation and/or creation in post-operative Fontan patients. Release of Calcium Ions by the Sarcoplasmic Reticulum One of the special features of the sarcoplasmic reticulum is that within its vesicular tubules is an excess of calcium ions in high concentration. Evaluation of a new hi pyridine inotropic agent-milrinone-in patients with severe conges tive heart failure.
Kliff, 25 years: Common features associated with stroke lesions include a large clot burden, figure 46. If the mixed venous blood sample is taken from the right atrium, inferior vena cava, coronary sinus, or similar sites, a falsely low or high value for arterio venous difference may result. However, the increase in tension that occurs during contraction, called active tension, decreases as the muscle is stretched beyond its normal length-that is, to a sarcomere length greater than about 2. Several other factors may contrib ute to graft failure, including the presence of poor inflow or outflow, low cardiac output, a hypercoagulable state, com promise of the graft owing to patients crossing their legs, or external compression of the graft by sclerosis and fibrosis (for example, from a scarred groin).
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





