
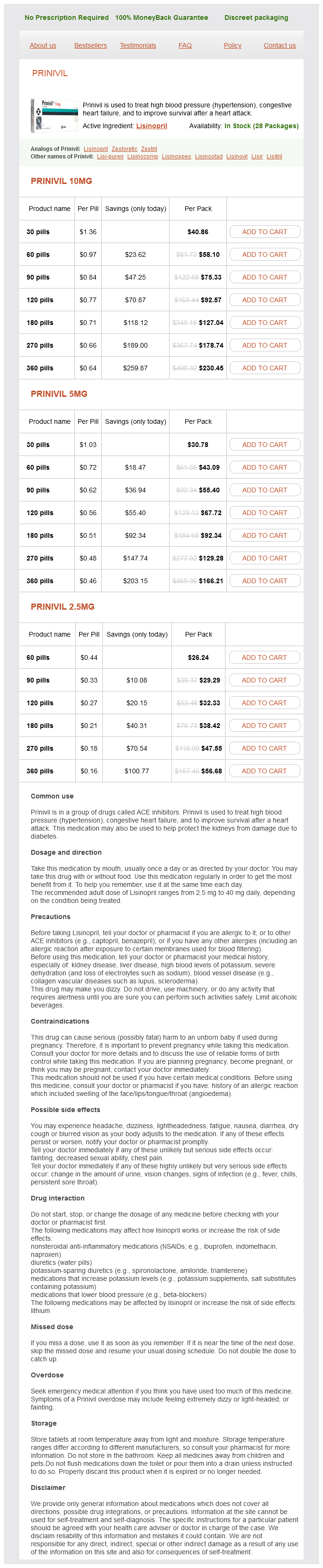
Prinivil dosages: 10 mg, 5 mg, 2.5 mg
Prinivil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 563
Only $0.17 per item
As a result blood pressure lying down prinivil 5 mg order on-line, T-cellmediated acute rejection has been become much less of a problem, while B-cellmediated responses such as antibody-mediated rejection and other effects of donor-specific antibodies have become more evident. In vitro and preclinical in vivo studies demonstrated that one can selectively inhibit immune responses to specific antigens without the associated toxicity of immunosuppressive therapies. With these insights comes the promise of specific immune therapies to treat an array of immune disorders from autoimmunity to transplant rejection (Riedhammer and Weissert, 2015). These findings gave rise to donor-specific transfusion protocols that improved outcomes. After the introduction of cyclosporine, however, these effects of blood transfusions disappeared, presumably due to the efficacy of this drug in blocking T-cell activation. Nevertheless, the existence of tolerance-promoting effects of transfusions is irrefutable. Tolerance Immunosuppression has concomitant risks of opportunistic infections and secondary tumors. Therefore, the ultimate goal of research on organ transplantation and autoimmune diseases is to induce and maintain immunological tolerance, the active state of antigen-specific nonresponsiveness (Krensky and Clayberger, 1994). Tolerance, if attainable, would represent a true cure for conditions discussed previously in this section without the side effects of the various immunosuppressive therapies. The calcineurin inhibitors prevent tolerance induction in some, but not all, preclinical models. In these same model systems, sirolimus does not prevent tolerance and may even promote tolerance (Kawai et al. In experimental animals, sirolimus promotes regulatory T cells, a subtype of T cells shown to suppress all immunity, and promotes tolerance. Studies in kidney transplant recipients showed that sirolimus spared regulatory T cells in the periphery, unlike calcineurin inhibitors, which reduced their percentage (Segundo et al. Dense meningeal infiltrates are found in the subarachnoid spaces of patients, and these infiltrates are intimately associated with subpial demyelination, neuronal and neuritic damage, oligodendrocyte loss, cortical atrophy, and parenchymal microglial activation in the outer cortical layers. Although each of these contributes only a small increase in the complex phenotype of disease risk, the biological functions associated with individual allelic variants have been striking. Many of these variants fall within specific signaling cascades, which suggests that alterations in pathways-rather than individual genes-may be useful in predicting response to therapy. The development of these antibodies, however, is on hold because of associated thromboembolic events. These antibodies are undergoing trials in non-Hodgkin lymphoma but are also likely to be developed for autoimmunity and transplantation. Donor Cell Chimerism A promising approach is induction of chimerism (coexistence of cells from two genetic lineages in a single individual) by first dampening or eliminating immune function in the recipient with ionizing radiation, drugs such as cyclophosphamide, or antibody treatment and then providing a new source of immune function by adoptive transfer (transfusion) of bone marrow or hematopoietic stem cells. On reconstitution of immune function, the recipient no longer recognizes new antigens provided during a critical period as "nonself. Specific therapies are aimed at resolving acute attacks, reducing recurrences and exacerbations, and slowing the progression of disability. The mAb natalizumab, directed against the adhesion molecule 4 integrin, antagonizes interactions with integrin heterodimers containing 4 integrin, such as 41 integrin that is expressed on the surface of activated lymphocytes and monocytes.
Dried Apricot (Apricot). Prinivil.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96915
It may take up to 12 h to develop analgesia and up to 16 h to observe full clinical effect blood pressure levels.xls prinivil 2.5 mg order without a prescription. Plasma levels stabilize after two sequential patch applications, and the kinetics do not appear to change with repeated applications (Portenoy et al. However, there may be substantial variability in plasma levels after a given dose. If excessive sedation or respiratory depression occurs, antagonist infusions may need to be maintained for an extended period. Dermatological side effects from the patches, such as rash and itching, usually are mild. Opiate-addicted patients have been known to chew the patches and receive an overdose, sometimes with fatal outcomes, following rapid and efficient buccal and sublingual absorption. Guidelines for Opiate Dosing the World Health Organization provides a three-step ladder as a guide to treat both cancer pain and chronic noncancer pain (Table 206). The three-step ladder encourages the use of more conservative therapies before initiating opioid therapy. Weaker opioids can be supplanted by stronger opioids in cases of moderate and severe pain. Antidepressants such as duloxetine and amitriptyline that are used in the treatment of chronic neuropathic pain have limited intrinsic analgesic actions in acute pain; however, antidepressants may enhance morphine-induced analgesia. In the presence of severe pain, the opioids should be considered sooner rather than later. There has been a growing concern over the appropriate use of opiates in pain management. Since the last edition of this textbook, there has been increasing scrutiny of the use of opioids to treat chronic pain due to the high correlation between prescription opioids and opioid abuse. Drug overdose has become the leading cause of accidental death in the Therapeutic Considerations in Pain Control Given its profound impact on patient physiology and quality of life, the management of pain must be an important element in any therapeutic intervention. By many hospital-accrediting organizations, and by law in many states, appropriate pain assessment and adequate pain management are considered to be standard of care, with pain considered the "fifth vital sign. Adjuvant agents are those that enhance analgesic efficacy, treat concurrent symptoms that exacerbate pain, or provide independent analgesic activity for specific types of pain. Acute Pain States In acute pain states, opioids will reduce the intensity of pain. However, physical signs (such as abdominal rigidity with an acute abdomen) generally will remain. In most cases, analgesics should not be withheld for fear of obscuring the progression of underlying disease.
On entry into host tissues blood pressure quizlet cheap prinivil 10 mg fast delivery, the first immune cells a pathogen encounters are the tissue-resident macrophages. Macrophages phagocytize microorganisms in a nonspecific fashion through their phagocytic receptors. Proteins of the complement system enhance this process by binding to receptors expressed by macrophages. In addition to engulfing invading pathogens, macrophages alert host cells of an infection. These cytokines recruit immune cells, the most prominent of which are neutrophils, to the infected tissue (Lavin et al. Mature neutrophils are kept in the bone marrow for up to 5 days before being released into circulation, ensuring a large reserve that can be summoned during an infection. Another receptor group, C-type lectin-like receptors, recognizes unique carbohydrate structures on invading microorganisms. Transcriptional induction of these immediate early response genes facilitates the establishment of an antiviral state, achieves antiproliferation in normal and tumor cells, and influences adaptive immune responses. Neutrophils die within 2 h of entry into infected tissues, forming the characteristic pus that develops at sites of infection (Kruger et al. Like neutrophils, these circulating leukocytes migrate from the blood to the site of infection in response to inflammatory cues. Adaptive Immunity Adaptive immunity refers to the arm of the immune response that changes (adapts) with each new infection. Following pathogen exposure, B and T cells with receptors that recognize the invading pathogen proliferate robustly and differentiate into effector lymphocytes. Soon after pathogen clearance, a large number of effector B and T cells die, but a small population of memory cells survives. Those cells have the ability to mount a rapid and specific response on reexposure to the same pathogen. This memory response, unique to adaptive immunity, is the basis for vaccination (see Chapter 36). This gene rearrangement enables the development of millions of pathogen receptors with unique binding sites, each expressed by a small subset of lymphocytes. Initiation of the Adaptive Immune Response the skin and mucosal surfaces prevent the majority of pathogens from entering host tissues and causing infections. Innate immune responses generally eliminate microorganisms that breach these barriers, typically within a few days. However, some pathogens establish an infection that cannot be controlled entirely by the innate immune response. Each polypeptide chain expresses an amino-terminal variable region, which contains the antigen-binding site, and a carboxy-terminal constant region.
Syndromes
Additional information:
Usage: p.o.
Tags: prinivil 10 mg sale, cheap 2.5 mg prinivil otc, buy 5 mg prinivil with visa, discount 2.5 mg prinivil with visa
Jorn, 41 years: In theory, therapeutic plasma concentrations of lidocaine may be maintained by intermittent intramuscular administration, but the intravenous route is preferred (Table 305).
Jerek, 30 years: The structure permits substitutions to be made on the aromatic ring, the - and -carbon atoms, and the terminal amino group to yield a variety of compounds with sympathomimetic activity.
Sobota, 39 years: In atrial flutter (panel E), the atria beat rapidly, approximately 250 beats/min (arrows) in this example, and the ventricular rate is variable.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





