
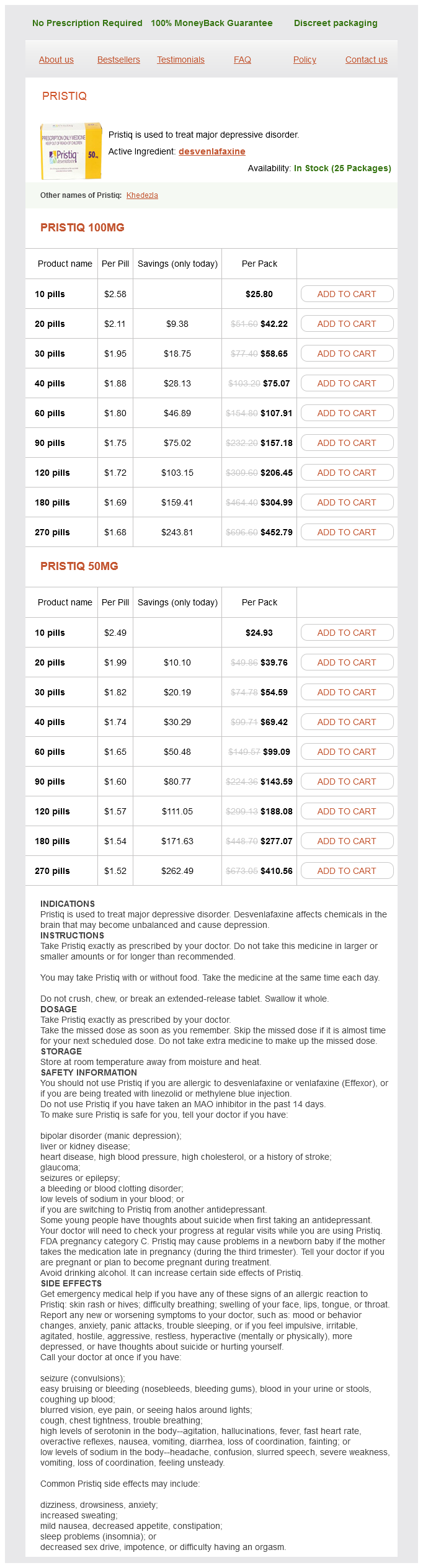
Pristiq dosages: 100 mg, 50 mg
Pristiq packs: 10 pills, 20 pills, 30 pills, 40 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 681
Only $1.62 per item
A number of dosing regimens have been described shinee symptoms mp3 generic 50 mg pristiq with mastercard, generally providing 2Â4 mg/kg daily or on alternate days for a total of 10Â15 doses. Pentamidine has also been used for chemoprophylaxis against African trypanosomiasis, with dosing of 4 mg/kg every 3Â6 months. Leishmaniasis-Pentamidine is an alternative to sodium stibogluconate and newer agents for the treatment of visceral leishmaniasis. The dosage is 2Â4 mg/kg intramuscularly daily or every other day for up to 15 doses, and a second course may be necessary. Important drugs that are not covered elsewhere in this or other chapters are discussed below. It leaves the circulation rapidly, with an initial half-life of about 6 hours, but is bound avidly by tissues. Hypoglycemia due to inappropriate insulin release often appears 5Â7 days after onset of treatment, can persist for days to several weeks, and may be followed by hyperglycemia. Few adverse effects occur initially, but the toxicity of stibogluconate increases over the course of therapy. Nitazoxanide appears to have activity against metronidazoleresistant protozoal strains and is well tolerated. Unlike metronidazole, nitazoxanide and its metabolites appear to be free of mutagenic effects. Other organisms that may be susceptible to nitazoxanide include E histolytica, Helicobacter pylori, Ascaris lumbricoides, several tapeworms, and Fasciola hepatica. The drugs are rapidly absorbed and distributed after intravenous (preferred) or intramuscular administration and eliminated in two phases, with a short initial (about 2-hour) half-life and a much longer terminal (> 24-hour) half-life. Treatment is given at a dosage of 20 mg/kg once daily intravenously or intramuscularly for 20 days in cutaneous leishmaniasis and 28 days in visceral and mucocutaneous disease. Their efficacy against different species may vary, possibly based on local drug resistance patterns. For visceral leishmaniasis, three new promising therapies are liposomal amphotericin, miltefosine, and paromomycin, and combinations of these agents have shown particularly promising results. Regimens that have been used include 1 g on days 1, 3, 7, 14, and 21 or 1 g each week for 5 weeks. Later reactions include fever, rash, headache, paresthesias, neuropathies, renal abnormalities including proteinuria, chronic diarrhea, hemolytic anemia, and agranulocytosis. Melarsoprol Melarsoprol is a trivalent arsenical that has been available since 1949 and is first-line therapy for advanced central nervous system East African trypanosomiasis, and second-line therapy (after eflornithine) for advanced West African trypanosomiasis. The most important toxicity is a reactive encephalopathy that generally appears within the first week of therapy (in 5Â10% of patients) and is probably due to disruption of trypanosomes in the central nervous system. Common consequences of the encephalopathy include cerebral edema, seizures, coma, and death.
Schizandra (Schisandra). Pristiq.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96390
An analysis of the p63/alpha-methylacyl coenzyme A racemase immunohistochemical cocktail stain in prostate needle biopsy specimens and tissue microarrays treatment diabetes type 2 order 50 mg pristiq visa. We prefer the term adenosis, as prefacing adenomatous hyperplasia with atypical has adverse consequences both in terms of practical patient management and in our theoretical framework of this entity. As outlined in the following text, there are very little data in support of a relation between adenosis and carcinoma. By designating these lesions as atypical, many patients will be subjected to unnecessary repeat biopsies. Included within the lower threshold are prostate specimens with foci of crowded glands, which could be considered a minimal example of adenosis, although they do not closely mimic adenocarcinoma. Crowded benign glands that have absent or patchy staining for basal cell markers and/ or positive racemase immunoreactivity are one of the more frequent mimickers of prostate cancer. The diagnosis of adenosis should be restricted to cases with a sufficiently atypical growth pattern that one has to seriously consider the diagnosis of low-grade cancer. This incidence is infrequent enough that many pathologists do not consider it in the differential diagnosis of small glandular lesions on needle biopsy. The distinction of adenosis from low-grade adenocarcinoma is based on architectural and cytologic features (Table 7. Note admixed more benignÂappearing glands with branching and papillary infolding adjacent to smaller crowded glands suspicious for cancer. Another common feature seen is the budding off of glands of adenosis from obviously benign glands. Glands of adenocarcinoma, even in the unusual case when the tumor is fairly lobular, shows a pure population of small crowded glands without benign architectural features that do not merge in with adjacent larger benign glands. In order for this feature to be diagnostically useful, the cytoplasm of benign prostate glands should appear pale or clear on routinely stained slides. A diagnosis of carcinoma should not be rendered based on what appears to be either a few individual cells or poorly formed glands within a nodule that is otherwise (text continues on p. Note admixture of more benignÂappearing glands with papillary infolding and branching adjacent to smaller crowded glands. Occasional single cells or poorly formed glands are not uncommon in a nodule of adenosis and probably represent tangential sections of small glands (Table 7. Usually, adenosis has been described as having totally bland-appearing nuclei without nucleoli. In contrast, the majority (70%) of foci of low-grade adenocarcinoma have occasional or frequent large nucleoli. The remaining low-grade carcinomas have either no prominent or at most rare prominent nucleoli.
An additional 20 mg of iron is needed each day for normal physiologic functions treatment canker sore cheap pristiq 100 mg without prescription, but the majority of this daily need is met through extracting iron during the process of recycling damaged red blood cell. It is interesting to note that there are no physiologic ways to excrete iron, and whatever iron is absorbed in the blood has to be either used or stored. Thus, the physiologic mechanisms of iron regulation focus on tightly controlling the absorption of iron from the small intestine. There are many proteins and cells involved in iron metabolism, but the major ones are shown in Table 15. They work as an integrated network to regulate iron absorption and to regulate blood and cellular levels of iron. This protein has an enormous capacity to bind iron and is a major physiologic storage form of iron. Transports iron out of cells (principally enterocytes and macrophages, also hepatocytes) into the bloodstream. Without hemojuvelin, these signaling pathways do not activate hepcidin gene synthesis in a normal fashion. In contrast, if the body has sufficient iron stores, then the iron is not transported into the blood but remains within the cytoplasm of the enterocytes. In healthy individuals, blood contains more transferrin protein than iron, with about 30% of the transferrin molecules saturated with iron. As blood iron levels increase, the excess transferrin protein serves as a reservoir that can quickly bind excess iron to prevent toxicity. However, if ferritin levels are excessive over a sufficiently long period of time, hemosiderin deposits can develop. Hemosiderin is composed of iron along with degraded ferritin and small amounts of other proteins. In contrast to the iron stored as ferritin, the iron in hemosiderin deposits is not readily available for biologic needs. In sum, two important iron reservoirs are used to keep blood iron levels at physiologically correct levels: (1) a short-term reservoir of iron stored within enterocytes and (2) a longer term reservoir of iron stored as ferritin, principally in hepatocytes and macrophages. If both reservoirs are unable to meet the demands for iron, then anemia develops; however, if iron control mechanisms are dysregulated. When hepcidin levels are lowered, more iron is absorbed from the gut and more iron is released into the blood. Hepcidin blocks iron transport by degrading ferroportin, the protein that exports iron out of cells into the blood. However, rare mutations have also been described that increase hepcidin function, with clinical manifestations of congenital refractory anemia. In contrast, hepatocellular carcinomas tend to have suppressed levels of hepcidin expression.
Syndromes
Additional information:
Usage: q.3h.
Tags: purchase pristiq 50 mg mastercard, pristiq 50 mg buy without prescription, cheap pristiq 50 mg without a prescription, cheap pristiq 50 mg buy online
Bufford, 24 years: The lobules show chronic inflammation that in most cases ranges from minimal or mild (55% of cases) to moderate (40% of cases).
Garik, 28 years: Diagnosis of a primary disorder usually requires further clinical and genetic data as well as ruling out secondary hyperlipidemias (Table 35Â3).
Akrabor, 53 years: When opiates are required, those with long half-lives or low addictive potential should be used.
Zapotek, 35 years: Blood testing may be used to document depressed activity of red blood cell (acetylcholinesterase) and plasma (butyrylcholinesterase) enzymes, which provide an indirect estimate of synaptic cholinesterase activity.
Marius, 60 years: Diagnosis of a primary disorder usually requires further clinical and genetic data as well as ruling out secondary hyperlipidemias (Table 35Â3).
Grim, 46 years: As blood iron levels increase, the excess transferrin protein serves as a reservoir that can quickly bind excess iron to prevent toxicity.
Bradley, 39 years: In contrast, if the tumor is clearly malignant, but you are not sure if it is metastatic, then stains for hepatic differentiation (shown in Table 20.
Lukar, 23 years: In addition, the histologic findings need to be correlated with the presence of preformed donor antibodies to confidently make the diagnosis.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





