
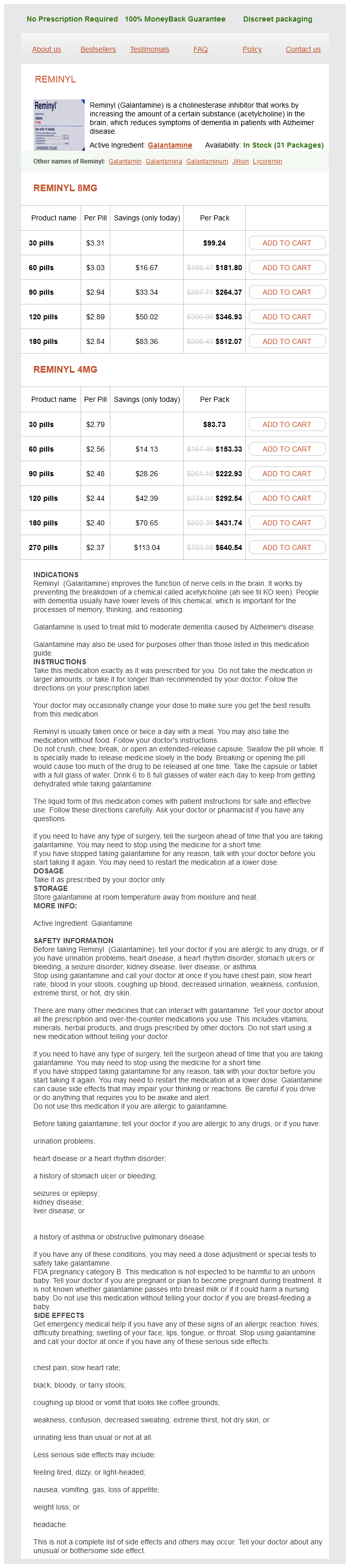
Reminyl dosages: 8 mg, 4 mg
Reminyl packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 736
Only $2.52 per item
This separation is dependent on normal blood flow medicine 81 cheap reminyl 4 mg line, which creates physical forces that tend to keep the heaviest cellular particles in the center of the vessel. As the rate of blood flow in the dilated vessels decreases in acute inflammation, the orderly flow of blood is disturbed. Penetration through the wall takes 2-10 minutes; in interstitial tissue, neutrophils move at a rate of up to 20 um/niin. Interaction between neutrophil surface receptors and these chemotaxins increases neutrophil motility (via an influx of Ca2+ ions, which stimulates contraction of actin) and promotes degranulation. Various cytokines (Chapter 4) play an increasing role as the immune response develops. Erythrocytes enter an inflamed area passively-in contrast to the active process of leukocyte emigration. Red blood cells are pushed out of the vessel by hydrostatic pressure through the widened intercellular junctions behind emigrating leukocytes (diapedesis). In severe injuries associated with disruption of the microcirculation, large numbers of erythrocytes enter the inflamed area (hemorrhagic inflammation). Recognition-The first step in phagocytosis is recognition of the injurious agent by the phagocytic cell, either directly (as occurs with large, inert particles) or after the agent has been coated with immunoglobulin or complement factor 3b (C3b) (opsonization). Opsonin-mediated phagocytosis is the mechanism operating in the immune phagocytosis of microorganisms. Immunoglobulin that is specifically reactive with antigens on the injurious agent (specific antibody) is the most effective opsonin. Early in acute inflammation-before the immune response has developed-nonimmune factors dominate, but as immunity develops, they are superseded by the more efficient immune phagocytosis. Engulfment-Once recognized by a neutrophil or macrophage, a foreign particle is engulfed by the phagocytic cell to form a membrane-bound vacuole called a phagosome, which fuses with lysosomes to form a phagolysosome. Microbial killing-When the offending agent is a microorganism, it must be killed before degradation can occur. Lysozyme was first discovered in tears by Alexander Fleming, who called it "tear antiseptic. Firmly stroking the forearm with a blunt instrument such as a pencil evokes the triple response: (1) Within 1 minute, a red line appears along the line of the stroke as a result of dilation of arterioles, capillaries, and venules at the site of injury; (2) simultaneously, a red flare develops as a result of vasodilation in the tissue surrounding the injury; and (3) a wheal forms because of exudation of fluid along the line of injury. The major components of acute inflammation-the red line and the wheal-were shown to be independent of neural connections in the tissue. This discovery laid the foundation for understanding the role of chemical mediators in acute inflammation. Many other chemical mediators have been discovered, but the exact role of individual mediators in inflamed tissue is unknown; their actions in vivo can only be postulated on the basis of their demonstrated in vitro activity. Vasoactive Amines: Histamine and serotonin are released from mast cells and platelets and can be identified early in the course of acute inflammation. Histamine is more important than serotonin in humans; it acts mainly on venules that have Hjhistamine receptors.
Potassium. Reminyl.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96824
Radiographic erosions or periarticular osteopenia in hand or wrist joints a Box 38 symptoms 6 dpo reminyl 4 mg lowest price. To be classified as having rheumatoid arthritis, a patient must meet at least four of the seven criteria. Joint pain is usually more prominent and more persistent than in osteoarthritis, occurring at rest, at night, and on activity. In addition to the symmetrical peripheral joint involvement, the cervical spine may also be involved. The synovium-lined atlantoaxial joint and/or the posterior apophyseal joints may become inflamed, causing pain in the neck and occipital headache. Uncontrolled disease eventually results in inflammation spreading beyond the synovium of the joint to other nearby structures, including the tenosynovium of tendons, ligaments, other soft-tissue structures, and bone. The distribution of radiologic disease in decreasing order of frequency is hands, feet, knees, hips, cervical spine, shoulders, and elbows. Considerable progress has been made in developing validated instruments to assess disease activity and severity, which in turn allow for appropriate provision and monitoring of therapy. Two methods using numeric scoring systems are currently employed and assess a number of parameters including numbers of swollen and tender joints, inflammation markers, and global health and quality of life assessments. Anemia, thrombocytopenia, leukopenia, or abnormal liver function tests may also be caused by drug toxicity. The earliest radiographic changes are seen in the hands in the form of soft-tissue swelling and periarticular osteopenia, but these are nonspecific signs. They reduce morning stiffness and the pain and swelling of inflamed joints but do not influence the acute-phase response or radiologic progression. Paracetamol (acetaminophen) with or without dextropropoxyphene, codeine, dihydrocodeine, or tramadol are all effective for symptom control. Efficacy cannot be predicted for an individual patient, but two-thirds of patients may respond. In another prospective three-year follow-up study of 119 patients with early disease, a nine-month delay in starting hydroxychloroquine resulted in a detrimental effect on pain intensity and patient global well-being. These agents target a variety of small molecules and can be differentiated into four main categories: 1. One recent study using combination therapy (including infliximab) demonstrated that in rheumatoid patients with less than two years of disease more than 50 percent were able to completely stop infliximab after one year of therapy, suggesting that medication-induced remission may be possible in some patients. They include skin rashes, mouth ulcers, altered taste, gastrointestinal reactions, proteinuria, bone marrow suppression, and autoimmunemediated disorders such as myositis and myasthenia gravis24[I] Adverse effects are common and include abnormal liver function tests, mouth ulcers, skin rashes, gastrointestinal, or hematological disorders. Other side effects include nausea, vomiting, abnormal liver function tests, and bone marrow suppression32[I] Nausea, vomiting, bone marrow suppression, alopecia, and increased risk of infection and cancer. Other adverse effects include nausea, dyspepsia, hypertrichosis, gingival hyperplasia, hepatic toxicity, and increased risk of infections and cancer. Serious adverse effects are rare36[I] Ocular complications, with the risk being higher with chloroquine than hydroxychloroquine. Other adverse effects include gastrointestinal disturbances (the most common), skin rashes, renal abnormalities, vertigo, blurred vision, and (Continued over) Chapter 38 Chronic joint pain] 523 Table 38.
The following definitions will be used: phantom pain: painful sensations referred to the missing limb; phantom sensation: any sensation of the missing limb medications on airline flights purchase 4 mg reminyl overnight delivery, except pain; residual limb pain: pain referred to the amputation residual limb. Very early studies claimed that the Prospective studies in patients amputated mainly because of peripheral vascular disease have shown that the onset of phantom pain is usually within the first week after amputation. In a retrospective study, however, of individuals who were either born limb-deficient or amputated before the age of six years, Melzack et al. Case reports confirm that the onset of phantom pain can be delayed for months or even years. In a survey of 526 veterans with longstanding amputations, phantom pain had disappeared in 16 percent, decreased markedly in 37 percent, remained similar in 44 percent, and increased in 3 percent of the respondents reporting phantom pain. In a survey of 526 veterans with a median time of 50 years since amputation, patients with phantom pain graded the intensity of pain as 5. In another recent study of 914 amputees, pain was classified into three categories: 38. In a prospective study of 52 amputees, the Chapter 31 Postamputation pain] 417 position of phantom pain within the phantom limb was in the toes or foot in 66. The following example illustrates some of the clinical characteristics of phantom pain. After the amputation, he suffered from severe phantom pain located to his hand and fingers. The phantom arm was located in front of the chest and the hand was clenched in a painful fist. Light touch of a trigger point in front of the ear resulted in exacerbation of phantom pain. Occasionally, massage of the residual limb loosened the fingers and allowed for voluntary movements. The hypothesis is that preoperative pain may sensitize the nervous system, thus making the individual very susceptible to the development of phantom pain. In traumatic amputees, phantom pain was only related to preamputation pain immediately after the amputation. However, some patients with severe preoperative pain never developed phantom pain, while others with traumatic amputations who never experienced pain before the amputation developed phantom pain to the same extent as patients with longstanding preamputation pain amputated for medical reasons. Acute postamputation pain intensity was the only significant independent predictor of chronic phantom pain at 6 and 12 months after amputation, whereas preamputation pain intensity was the only significant predictor of chronic phantom at 24 months. Some amputees lost their limbs at the time of the initial injury (immediate, 56 percent); others suffered a severe injury and had a subsequent limb amputation at hospital on average ten days after the injury (delayed, 44 percent).
Syndromes
Additional information:
Usage: p.r.n.
Tags: safe 8 mg reminyl, purchase reminyl 4 mg on line, 4 mg reminyl buy with amex, 8 mg reminyl buy free shipping
Boss, 51 years: Studies using whole-genome (genome-wide) scanning approaches in uncovering genes for pain are under way. In complete biliary obstruction, absence of bilirubin alters the normal color of the feces (producing clay-colored stools).
Raid, 43 years: Neoplasms of totipotent cells (germ cell neoplasms, bottom), compared with the development of the normal zygote (top). Spasm of the sigmoid colon, levator ani, and/or pelvic floor musculature have been postulated as sources of the pain.
Sivert, 40 years: Comparison of the efficacy and tolerability of a paracetamol/codeine fixeddose combination with tramadol in patients with refractory chronic back pain. In order for the test to be positive, reproduction of pain upon testing one disk must be accompanied by no pain when adjacent disks are tested.
Steve, 26 years: Screening tools are now available to supplement the clinical impression and similarly, instruments now exist to identify when problems are occurring. Any particle that is coated with immunoglobulin or complement (ie, opsonization has occurred) is phagocytosed more readily than naked, uncoated, particles (see Chapter 3).
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





