
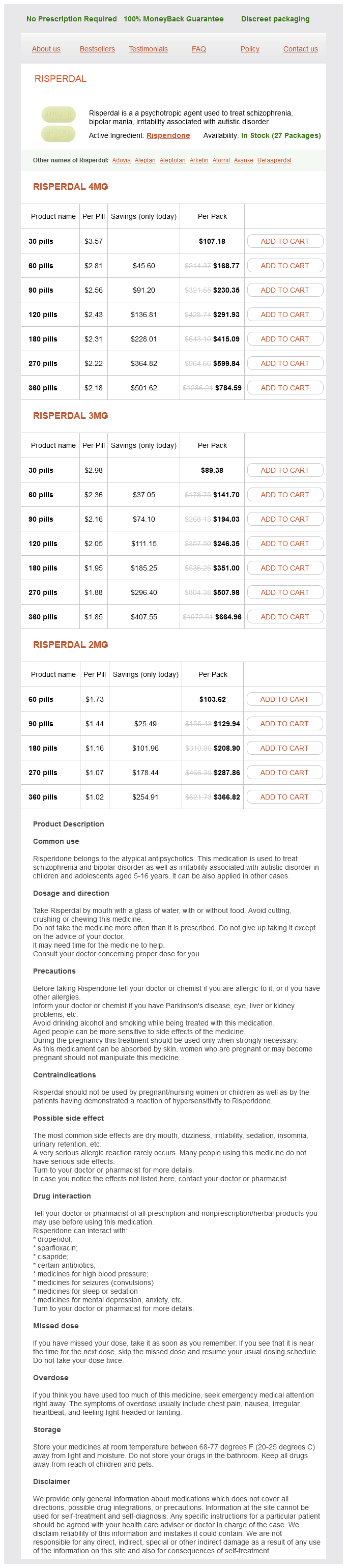
Risperidone dosages: 4 mg, 3 mg, 2 mg
Risperidone packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 871
Only $1.08 per item
All neonates with seizures should have a trial of pyridoxine and folinic acid treatment if the cause is not identified and seizures persist medicine hat horse 3 mg risperidone purchase with amex. Plasma amino acids and urine orotic acid can help define the specific urea cycle defect Elevated urine and plasma glycine levels, normal organic acid pattern and ammonia level. Both these disorders can manifest later in childhood with developmental delay and episodic symptoms such as ataxia and vomiting Refractory seizures, rash, alopecia; lactic and organic acidosis Onset in infancy with developmental delay and seizures; seizures occur in about 25%, and the infant may have severe epilepsy with West syndrome; deficiency of phenylalanine hydroxylase causes the accumulation of phenylalanine and phenylacetic acid Biotinidase deficiency Aminoacidurias Phenylketonuria Nearly 100% identified through New Born Screening. Dysmorphic features and skeletal changes similar to Morquio mucopolysaccharide storage disorder A clinical syndrome resulting from various abnormalities of mitochondrial oxidative phosphorylation Usually manifesting in infancy with regression of motor skills, hypotonia, lethargy, respiratory disorders (typically hyperventilation and apnea), and seizures; other features are nuclear and supranuclear oculomotor paralysis, brainstem dysfunction, choreoathetosis, cerebellar ataxia, and pyramidal signs Sex-linked inheritance on long arm of X chromosome; hypotonia, failure to thrive, abnormal temperature regulation, hypothermia or hyperthermia, fragile wiry hair, poor pigmentation, generalized seizures, often infantile spasms Appears before 3-6 mo of age; rigidity develops in an irritable, crying infant; opisthotonic posturing of the neck and trunk; generalized motor seizures may occur, but must be distinguished from tonic spasms; affected children become blind with optic atrophy Developmental delay from birth, characteristic facies, ataxia with jerky limb movements, inappropriate laughter ("happy puppet"), seizures in 86% of patients 523 Investigations Nearly 100% identified through New Born Screening. Four known genetic mechanisms can cause Angelman syndrome; approximately 70% of cases result from de novo maternal deletions involving chromosome 15q11. Pyridoxine-dependent seizure is a rare autosomal recessive disorder in which seizures usually appear within the first 3 months of life, often within hours of birth, but in rare cases, as late as 2-5 years of age. Folinic acid-responsive seizures present very similarly to pyridoxine-dependent seizures, with medically intractable, relentless seizures of multiple types, often within the first days of life. These are rare disorders, but as they are neurologically devastating or fatal if untreated, it is reasonable to administer a trial dose of pyridoxine and/or folinic acid to seizing, encephalopathic infants where no other cause has been found for their seizures and encephalopathy. If there is a clinical, and ideally electrographic, response to the vitamin trial, then it is also reasonable to continue the supplement. Nonetheless, even with early diagnosis and treatment, these children may have developmental delays. Although these abnormalities are present from birth, seizures may develop at any age. Lissencephaly, or agyria, is a profound abnormality characterized by a smooth brain without development of the normal gyral pattern and sulci; there are often large heterotopia in the white matter, and neuroimaging studies may reveal the appearance of a double cortex. Hemimegalencephaly is characterized by gross enlargement of 1 hemisphere with no normal cortical development within that hemisphere. More restricted abnormalities may occur in the form of a limited area of gyral enlargement and distortion called pachygyria. Schizencephaly refers to unilateral or bilateral clefts in the cerebral hemispheres, usually with abnormal arrangement (polymicrogyria) of the cortical gray matter lining the clefts. Porencephalic cysts communicate with both the subarachnoid space and the ventricular system and are lined not by cortical gray matter but rather by white matter because they result from loss of tissue as a consequence of insults, typically infarction or hemorrhage, during development. Early myoclonic encephalopathy appears in neonates before 2-3 months of age, usually within the first 2 weeks of life. There is a failure or arrest of psychomotor development and a high rate of mortality before 12 months of age. A number of patients have an inborn error of metabolism, including nonketotic hyperglycinemia, D-glyceric acidemia, propionic acidemia, and methylmalonic acidemia. Affected children have a severe encephalopathy, and the prognosis for remission from seizures or for normal development is very poor. Infancy the paroxysmal disorders of infancy (8 weeks to 2 years) are shown in Tables 30.
Geranien (South African Geranium). Risperidone.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97079
Second Heart Sound Shortly after the onset of ventricular contraction symptoms 5th week of pregnancy risperidone 2 mg order with visa, the semilunar valves (aortic and pulmonary) open and permit ventricular ejection. As ventricular ejection nears completion, the pressure begins to fall within the ventricles, and the semilunar valves snap closed. This prevents regurgitation from the aorta and pulmonary artery back into the heart. The S2 usually consists of a louder and earlier aortic valve closure sound (A2), followed by a later and quieter pulmonary valve closure sound (P2). Normal physiologic splitting or variability is appreciated most easily in the pulmonary area during or near the end of inspiration. During expiration, the aortic and pulmonary valves close almost synchronously and produce a single or narrowly split S2. Normal splitting of S2 is caused by (1) increased right-sided heart filling during inspiration because of increased blood volume returning via the venae cavae; and (2) diminished left-sided heart filling because blood is retained within the small blood vessels of the lungs when the thorax expands. During inspiration, when the right ventricle is filled more than the left, it takes slightly longer to empty. Splitting of the S2 during inspiration is a normal finding and should be sought in all patients. Many forms of congenital or acquired heart disease have an impact on the pulmonary circulation and, consequently, often affect the S2. Thus, the higher the pulmonary artery diastolic pressure, the more intense and earlier the P2 is. Pulmonary hypertension in children is suggested when the P2 is palpable, loud, and narrowly split or cannot be separated from A2. If the P2 is audible outside of the pulmonary area, particularly at the apex, then pulmonary hypertension is likely. In the presence of moderate to severe pulmonic stenosis, there is low pulmonary artery diastolic pressure. The pulmonary valve closure is therefore delayed and of decreased intensity and is occasionally inaudible. When the ejection sound occurs at the upperright sternal border or at the apex, a bicuspid or stenotic aortic valve disease is suggested. In contrast to ejection clicks, right-sided cardiac murmurs are accentuated with inspiration. Left-sided heart auscultatory abnormalities vary little with the respiratory cycle. In the case of the aortic ejection click, the sound is usually well separated from S1.
In the event of severe acute blood loss shinee symptoms quality risperidone 4 mg, the newborn may present with signs of acute illness *Clinical manifestations with sickle cell trait are unusual but include renal papillary necrosis (hematuria), sudden death on exertion, intraocular hyphema extension, and sickling in unpressurized airplanes. The degree of anemia is highly variable, and the reticulocyte count is elevated in most patients; however, a minority of patients present with a low reticulocyte count because of immune destruction of reticulocytes. Congenital leukemia is a rare disorder characterized by infiltration of the bone marrow leading to anemia, thrombocytopenia, and leukocytosis in association with hepatosplenomegaly and occasionally cutaneous leukemic infiltrates manifesting as blue papular lesions ("blueberry muffin" spots). Infants with Down syndrome may present with a clinical and hematologic picture identical to that of congenital leukemia, which is a transient myeloproliferative process that spontaneously remits over several months. Infantile osteopetrosis (marble bone disease), a disorder characterized by a limited ability to degrade bone, usually does not cause pancytopenia until a few months after birth. Infants with hereditary spherocytosis, pyropoikilocytosis, or elliptocytosis may develop anemia and extreme hyperbilirubinemia that necessitates phototherapy and, rarely, exchange transfusion. Isoimmune hemolytic anemia is the most common cause of hemolytic anemia in the newborn. It is caused by incompatibility including lethargy, tachycardia, hypotension, and respiratory distress. The hemoglobin value is a poor index of the severity of acute blood loss because equilibration of fluid compartments may take 24-36 hours. Blood loss as a cause of anemia should always be suspected in cases of obstetric complications, multiple births, or difficult and traumatic deliveries. In the neonate who is hemodynamically stable but has experienced significant blood loss, a more conservative approach is recommended. In Rh incompatibility, the mother is Rh negative and the infant is Rh positive (inherited from the father). If the mother has been exposed to Rh-positive blood cells through prior pregnancy, miscarriage, therapeutic abortion, or mismatched blood transfusion, IgG antibodies may develop that traverse the placenta and cause immune destruction of fetal Rh-positive cells. In severe circumstances the fetus may be extremely anemic, which results in heart failure, hydrops fetalis, and death. In less serious instances infants may be born quite anemic and develop brisk hyperbilirubinemia, which can lead to kernicterus. The severity of Rh immune hemolytic disease increases with successive pregnancies. This disorder is uncommon because of the routine practice of administering Rh immunoglobulin to Rh-negative mothers who are 28-30 weeks pregnant and within 72 hours of delivery or after spontaneous or therapeutic abortion. Prenatal management of the affected fetus may include spectrophotometric assessment of amniotic fluid as an assessment of fetal bilirubin level and in high-risk situations serial fetal hemoglobin levels obtained by ultrasonographically guided aspiration of umbilical cord blood (cordocentesis). When the fetus demonstrates progressive in utero severe anemia, intrauterine intravascular blood transfusion therapy has been shown to decrease the risk for fetal demise.
Syndromes
Additional information:
Usage: p.c.
Tags: risperidone 2 mg low cost, risperidone 3 mg order with mastercard, discount 3 mg risperidone, order risperidone 2 mg fast delivery
Jose, 58 years: Incomplete Isosexual Precocity (Precocious Pseudopuberty) Precocious pseudopuberty refers to gonadal or adrenal sex-steroid secretion not resulting from activation of the hypothalamic-pituitarygonadal axis (pituitary-independent). It is more likely that a Salter Harris type I separation of the distal fibular epiphysis has occurred, rather than a true ligament injury. The liver also increases in size as a result of hepatic tumors, benign cysts, and infiltration of inflammatory or malignant cells. Ultrasound including the bladder should be performed to rule out other lesions discussed earlier.
Dargoth, 49 years: The child who has always appeared somewhat pale but is otherwise well with normal growth and development likely has an intrinsic constitutional characteristic. Laboratory Tests In an ill-appearing child, basic laboratory testing including complete blood count with smear; chemistries; blood, and possibly cerebral spinal fluid cultures should be obtained. Deficient clotting factors and platelets should be transfused to prevent further development of thrombosis or bleeding during anticoagulation. When severe acute blood loss occurs, intravascular volume depletion is the primary concern, which cannot be assessed by hemoglobin level.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





