
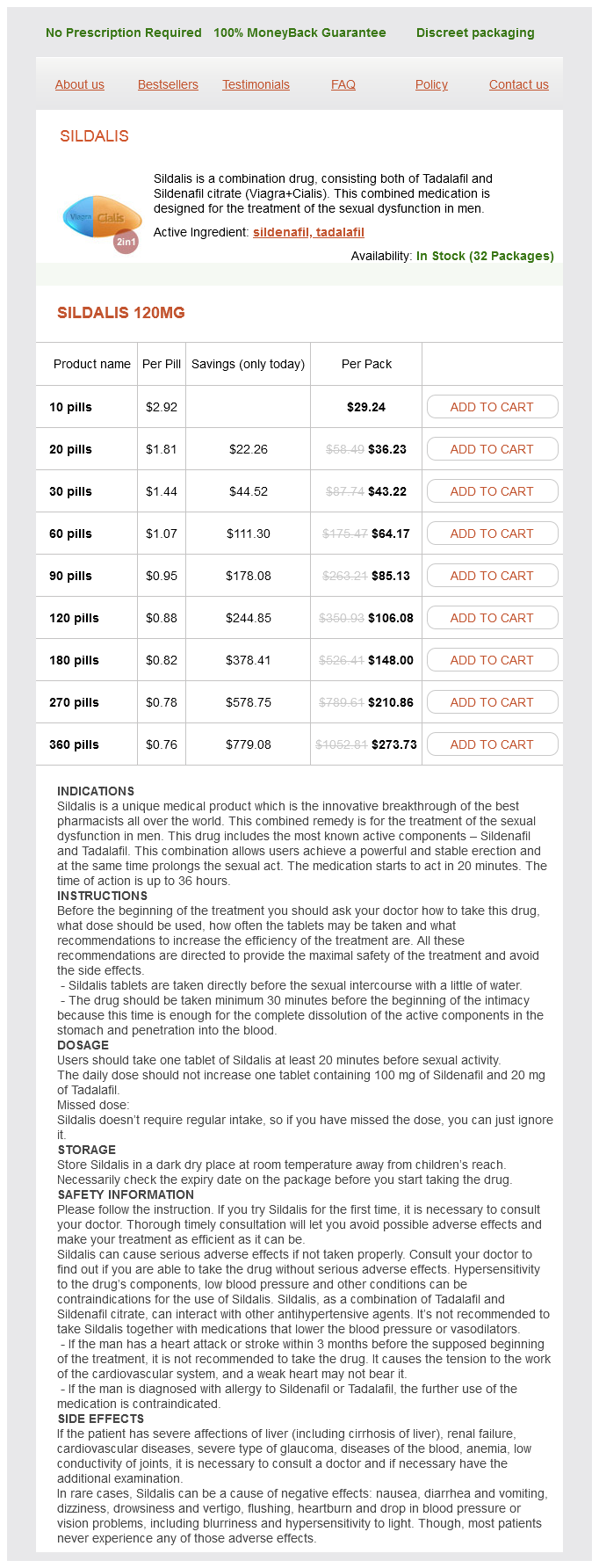
Sildalis dosages: 120 mg
Sildalis packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 780
Only $0.81 per item
The intramedullary veins erectile dysfunction acupuncture purchase sildalis 120 mg online, which drain the spinal cord parenchyma, empty into surface veins, including dorsal, sulcal, and ventral spinal cord veins. Two longitudinally oriented veins, the posterior spinal and anterior medial spinal veins, are valveless and drain through the radicular veins into the extradural venous plexus. Upon dural penetration, functional valves are formed at the level of the radicular veins, preventing retrograde flow from the epidural vertebral veins into the intradural extrinsic system. Classification of Vascular Spinal Lesions Key Concepts Spinal vascular lesions are rare but are associated with significant morbidity. Spinal vascular lesions are rare, underdiagnosed, and poorly understood entities that, if not treated promptly and adequately, could cause progressive spinal cord injury and myelopathy. Depending on the lesion type, symptoms vary between acute intramedullary/subarachnoid hemorrhage and subacute venous hypertension. Multiple classifications considering biological features, location, and genetic predisposition have been proposed. Although it might be primarily asymptomatic, enlargement of the veins could cause mass effect on the adjacent nerve roots and spinal cord. These rare fistulas are primarily treated by endovascular techniques that aim to close the fistula. They are composed of a radicular feeding artery communicating with the dorsal coronal venous plexus at the spinal cord. The fistula point is typically in the nerve root dural sleeve and primarily obstructs venous outflow of the cord, leading to venous hypertension and myelopathy. Histologically, they are composed of subpial shunts and may be compact or diffuse, based on the angioarchitecture of the nidus. Both endovascular and surgical treatments may be useful, although resection carries the advantage of removing mass effect. In addition to the spinal cord and nerve roots, the bone, paraspinal muscles, and skin of a given metamere are also affected, although symptoms are mostly due to the intramedullary component. Multiple palliative endovascular treatments are the norm for this complex condition, which is mostly diagnosed in young adults. Depending on size, they can be divided into type A (single small feeder), type B (several feeders at the level of the fistula), and type C (giant multipediculated lesion with massive dilated venous channels). Anterior/anterolateral surgical approaches are preferred for type A lesions, given the risk of catheterizing and embolizing the anterior spinal artery. Identify arterial feeders and their relationship with radiculomedullary (particularly artery of Adamkiewicz) and radiculopial arteries that are not feeding the fistula. Identify the presence of aneurysms and venous varices and their relationship with the symptoms. Transarterial embolization combined with surgical decompression of the cauda equina can result in a good outcome. Other spinal vascular masses include benign tumors (hemangioma, hemangioblastoma, aneurysmal bone cyst, osteoid osteoma, osteoblastoma), malignant tumors (multiple myeloma, plasmacytoma, hemangiopericytoma, giant cell tumor, chondrosarcoma, osteogenic sarcoma), certain metastatic tumors (renal cell and thyroid carcinoma), and cavernous malformations. Mario Martinez-Galdamez, Director, Interventional Neuroradiology Unit, Department of Radiology, University Clinic Hospital of Valladolid, Spain.
PMF (Methoxylated Flavones). Sildalis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97032
Scalp: All five layers of the scalp (skin erectile dysfunction doctors los angeles generic sildalis 120 mg buy on-line, subcutaneous tissue, galea aponeurotica, underlying loose areolar tissue, and the skull periosteum) are injured even in superficial and tangential injuries. Subperiosteal hematomas can occur in children,whereas subgaleal hematomas, that is, not confined by sutures, are more common in adults. Bone: the angle of impact and regional differences in skull thickness influence the severity of the fracture and brain injury. Fracture pattern and bone beveling may distinguish entry and exit sites, which have both clinical and medical-legal implications. Irregular stellate fractures that radiate from the point of impact are seen at the entry site; the inner table is usually more comminuted than the outer table. Where there is an exit wound, there are shorter fracture lines and the outer table may be more comminuted than the inner table. These in-driven bony fragments may cause additional injury and pose management challenges when near a venous sinus. Intracranial contents: When the pia and arachnoid are torn, cerebral laceration occurs. This usually results in a conical lesion with the base at the entrance and the laceration tapering inwards along the projectile tract. Both can contribute to reduced cerebral perfusion pressure and infarction with or without herniation. Pharmacological paralysis should be avoided and reversed if necessary to obtain an examination. Entry and exit wounds should be assessed, including the presence of contact burns, which may be important in determining trajectory and proximity of gun to the cranium. The cervical spine should be immobilized, but if there is no evidence for injury, further immobilization is not necessary. Many patients have lost large amounts of blood before reaching the emergency department or may present with acute coagulopathy of trauma/shock. Consequently, determining the hemoglobin concentration, coagulation profile and platelet count, and a type and cross-match is important. Coronal and sagittal views are helpful for patients with skull base or craniofacial involvement or high convexity injuries. Endovascular treatment of exsanguinating hemorrhage is sometimes required for injuries to major extracranial and/or intracranial vessels. Procedure Key Concepts the primary goal of surgery is to eliminate mass effect and preserve remaining viable tissue. Secondary goals are to remove bone and missile fragments and close the dura and scalp. There are three broad indications for surgery: 1) hematoma evacuation; 2) control of mass effect; and 3) restoration of dural, craniofacial, and scalp integrity for infection control.
Fiberoptic examination of the airway reveals paradoxical movement (medial displacement) with inspiration erectile dysfunction treatment in thailand order 120 mg sildalis visa. Immediate treatment options include medical treatments to decrease airway edema, intubation, and tracheostomy. Options for medical management of airway edema include supplemental oxygen, proper positioning, nebulized racemic epinephrine, dexamethasone, and inhaled Heliox (Table 43. Posterior drainage into the nasopharynx may induce coughing, which should raise suspicion for a leak. If suspected, a small sample of fluid should be collected and tested for beta-2transferrin, which has higher sensitivity and specificity than traditional glucose testing. These symptoms could mimic the symptoms of meningitis, thus clouding the picture and potentially having a negative impact on medical decisions. Prompt reexploration is preferred over lumbar drainage after endonasal skull-base surgery, given the size of potential defects and lack of intervening tissue. Volume of drainage must be monitored closely because overdrainage can occur and produce pneumocephalus, low-pressure headaches, nausea, vomiting, vocal cord paralysis, and even obtundation. In addition, other problems encountered include fracture and retention of drain fragments, chemical meningitis, hemorrhage, occlusion of the posterior cerebral artery, and lumbar radiculopathy. Material Allograft Nonvascularized autograft Vascularized flap Technique Flap harvest Inlay graft Flap placement Packing Perioperative Care Lumbar drain Debridement Patient activity Packing Pneumocephalus the incidence of air in the cranial vault, or pneumocephalus, is rare after endoscopic sinus surgery or microscopic skull-base surgery. Symptoms reported with pneumocephalus include mental status changes, new or worsened headache, nausea, vomiting, and seizures. Some degree of pneumocephalus is to be expected after cranial base surgery that includes opening of the dura; gradual resolution over a week is to be expected. Treatment of pneumocephalus after skull-base surgery should initially be managed with conservative measures such as bed rest, head elevation, supplemental oxygen via a face tent or 100% nonrebreather with absolute avoidance of positive pressure, and pain control. In severe or persistent cases, diversion of the airway with intubation or tracheostomy may be necessary. Reconstruction Failure of reconstruction of the skull base can result in any of the previously mentioned complications. If a patient has a free flap for reconstruction, there are typically very tightly controlled hemodynamic criteria applied. In addition, the type of pressor or antihypertensive agent used should be carefully considered given its potential effects on cerebral or flap arterial supply. Visual Deterioration Endoscopic endonasal and skull-base surgeries can produce visual deficits through injury to the optic nerves, ischemia, or hematoma formation. Visual loss can occur as a result of complications anywhere along the visual pathways after skull-base surgery. Chiasmal compression from postoperative intracranial hematoma will result in a bitemporal hemianopsia.
Syndromes
Additional information:
Usage: p.c.
Tags: buy discount sildalis 120 mg online, purchase sildalis 120 mg, 120 mg sildalis buy amex, discount sildalis 120 mg line
Bandaro, 26 years: Therefore the single high dose delivered during radiosurgery is thought to preferentially lead to cytotoxicity over mutagenicity. Tumors of the foramen magnum often displace or encompass the vertebral artery, increasing the potential for vascular injury and the need for possible arterial sacrifice in order to achieve complete resection.
Marus, 60 years: Nonantibiotic preventative strategies, including methenamine hippurate, can be tried. Scalp: All five layers of the scalp (skin, subcutaneous tissue, galea aponeurotica, underlying loose areolar tissue, and the skull periosteum) are injured even in superficial and tangential injuries.
Nerusul, 65 years: Current dialysate delivery technology requires the preparation of two separate dialysate streams, one called "acid concentrate," which combines all the ingredients of dialysate except sodium bicarbonate, and a second stream that contains sodium bicarbonate and sodium chloride. Majority of microvascular events occur in the first 48 hours after initial procedure.
Brant, 42 years: Given the association of both hypoglycemia and hyperglycemia with poor outcomes in neurosurgical patients, the goal of anesthetic management is to maintain normoglycemia. Relatively normal proximal tubular cytoplasm stains red in the tubules on the left and at the bottom.
Thorus, 55 years: Primary tumors of this area may be derived from bone, paranasal sinuses, nasopharynx, dura, cranial nerves, pituitary gland, meninges, and brain. The collection can compress the brain and cause neurological deficits, headache, and decreased consciousness.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





