
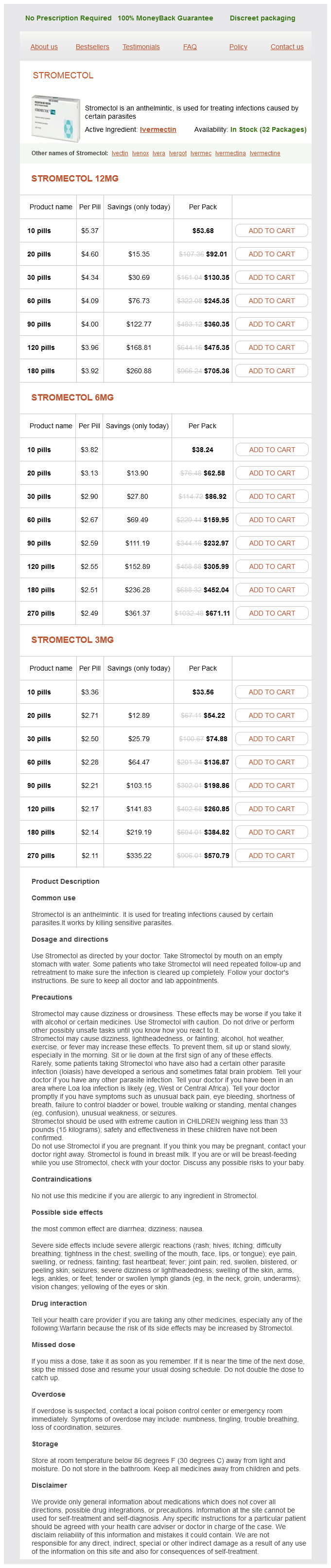
Stromectol dosages: 12 mg, 6 mg, 3 mg
Stromectol packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 848
Only $2.25 per item
Where possible antibiotic resistance fact sheet best stromectol 3 mg, the left ventricle is connected to the aortic valve via a baffle, and outflow tract obstruction is relieved. The right ventricular communication with the main pulmonary is restored using the required combination of subpulmonary resection, pulmonary valvuloplasty/patch annuloplasty, or right ventricular to pulmonary artery conduit. If the pulmonary outflow is minimally obstructed, an arterial switch may still be performed; however, more significant obstruction must be dealt with differently. First, if the pulmonary outflow is not critically obstructed, balloon atrial septostomy to improve mixing of oxygenated and deoxygenated blood at atrial level may leave the patient sufficiently saturated to be followed as an outpatient for weeks and sometimes months. Patients without severe obstruction are likely to be asymptomatic in the perinatal period and can be discharged for outpatient follow-up. In this group, an early operative procedure may be necessary to alleviate cyanosis and/or pulmonary congestion. Others may require a balloon atrial septostomy to increase intracardiac mixing, which results in more deoxygenated blood being ejected into the pulmonary artery. If the ductus becomes restrictive or closes, femoral pulses will be reduced or absent, and the infant is at risk of developing shock. Conversely, an unobstructed pulmonary outflow could lead to the simultaneous development of congestive cardiac failure in the setting of cyanosis and poor femoral pulses. Long-term risks include the need for reintervention for the aortic arch, and the pulmonary outflow tract due to progressive obstruction at subvalvar, valvar, and supravalvar levels. Cases with associated ventricular hypoplasia usually follow a single ventricle pathway, with early palliation in the form of a systemic to pulmonary artery shunt in the setting of severe pulmonary outflow tract obstruction, or pulmonary artery band in those with unobstructed pulmonary blood flow. Close follow-up is required for cases with less severe pulmonary outflow tract obstruction. In all cases, a subsequent bidirectional cavopulmonary shunt and a Fontan are performed. In population-based studies from countries with well-developed fetal screening programs, the rate is about 60%, and up to 78% has been reported where national fetal cardiac screening is implemented. Improvements in diagnostic accuracy occur with multiple prenatal examinations,13 and the type of surgery required can be predicted in 90% of cases. Situs the position of the fetus in the uterus should first be established, and left and right sidedness determined. In cases of right isomerism, a more posterior stomach position may be a clue to the presence of associated asplenia. Four-chamber view Ventricles: Ventricles should be identified according to morphological criteria. Sweeps through the heart are particularly useful to correctly identify relationships of structures. The right ventricle, in this context, is on the left side of the heart, and a ventricular septal defect is present. The great arteries are often configured more akin to L-transposition with an anterior and leftward aorta.
Fishfudle (Jamaican Dogwood). Stromectol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96531
In duct-dependent systemic blood flow antimicrobial zone of inhibition evaluation stromectol 3 mg buy low price, compromise of systemic perfusion occurs with ductal constriction. The right ventricle pumps both the systemic and the pulmonary venous return into the pulmonary artery, pulmonary arterial branches, and via the ductus arteriosus to the aorta. Progressive narrowing of the ductus arteriosus, which is the only pathway to the systemic circulation, leads to a fall in the blood pressure and underperfusion of the central and peripheral organs, including the coronary circulation. Tachypnea, hypotension, pronounced acidosis, and moderate cyanosis may lead to the (a) 60/35 80 61 Ao 80 erroneous presumptive diagnosis of neonatal sepsis or metabolic disorder. Progressive ductus arteriosus occlusion leads to progressive decrease in systemic circulation, resulting in acute coronary hypoperfusion, shock, multiorgan failure, and eventually death. Early use of prostaglandin derivatives can prevent ductal occlusion for a limited period of time. The functionally single right ventricle serves the pulmonary and systemic circulation. The proportion of the ventricular output that goes to the pulmonary or systemic vascular bed is determined by the relative resistance to flow within the two circuits. As the pulmonary resistance continues to drop, more blood preferentially reaches the pulmonary circulation (Qp) than the systemic circulation (Qs). Pulmonary venous return enters the right heart through the mildly restrictive foramen ovale. The resultant arterial O2 saturation of 75%80% represents balanced pulmonary and systemic blood flow (Qp:Qs = 1). Therefore, intensive medical interventions aim to recognize duct-dependent heart defects as early as possible, as well as regulate pulmonary and systemic perfusion. Clinical signs are progressive cyanosis within a few hours of birth as the patent ductus arteriosus constricts, which does not improve following treatment with oxygen (hyperoxia test). Congenital heart disease with duct-dependent mixing the simple transposition of the great arteries is characterized by parallel arrangement of both circulations: the highly saturated pulmonary venous return reaches the left ventricle and recirculates via the pulmonary artery into the lung; the low saturated systemic venous return reaches the right ventricle, is ejected into the aorta, and recirculates throughout the body. Pulmonary blood flow is served by the left ventricle via the aorta and the ductus arteriosus which has a typical vertical shape. The systemic venous return drains across the open foramen ovale into the left atrium (right-to-left shunt). There is no antegrade flow across the pulmonary valve, and the right ventricle is decompressed by tricuspid regurgitation. Arterial O2 saturation reflects mixing between pulmonary and systemic circulations. The oxygen saturation of the aorta is similar to the right ventricle, and hence, the neonate appears deeply cyanotic. Although shunting across the patent ductus arteriosus is typically bidirectional, only left-to-right-shunting across the foramen ovale allows highly saturated blood to reach the ascending aorta and through it the coronary circulation as well as head and neck vessels. Enlarging the atrial communication by balloon atrioseptostomy allows an increase in left-to-right shunt across the foramen ovale and significant increase in aortic oxygen saturation. A prenatal increase in the pulmonary vascular resistance, as seen in cases of intrauterine constriction of the ductus arteriosus or a restrictive interatrial communication in hypoplastic left heart syndrome,19 causes hypertrophy of the media of the pulmonary vessels prenatally and severe pulmonary hypertension postnatally.
The left aortic arch (A) and left pulmonary artery (asterisk) course above the left main bronchus antibiotic resistance marker genes cheap stromectol 3 mg buy line. Both pulmonary arteries (asterisks) are seen to course above the ipsilateral bronchi. Although it is possible to demonstrate the anatomy, the practical usefulness of this is questionable. One is the aorta and the other is the dilated azygos vein in this case of left isomerism. In most cases, the spleen is either absent (asplenia), or multiple spleens are present on the right or on the left (polysplenia). Generally, asplenia occurs with right bronchopulmonary and atrial isomerism, while polysplenia occurs with left bronchopulmonary and atrial isomerism. However, polysplenia can occur with right isomerism, and asplenia with left isomerism. While splenic morphology is somewhat variable, there is tighter concordance between bronchopulmonary situs and atrial situs so that the bronchopulmonary arrangement usually reflects the atrial arrangement. There is evidence to suggest that heterotaxy may have a genetic etiology,13,27,45,4953 although genetic anomalies were unusual diagnoses in our institutional experience46 with heterotaxy patients. Similarly, other studies have not found that there is a significantly increased risk for chromosomal abnormalities in heterotaxy. Moreover, left isomerism may be found incidentally without any clinical evidence of a cardiac defect. Nonetheless, there is considerable overlap in the cardiac malformations within the two types of isomerism (Table 17. In right isomerism more than left isomerism, the atrioventricular septal defect is usually characterized by an unbalanced commitment of the atrioventricular Table 17. The pulmonary artery is much smaller than the aorta (A) because of severe pulmonary stenosis. The atrium is a common chamber with a small strand of remnant atrial septum seen as a dot (central dot sign). In right isomerism, cardiac lesions are typically complex and usually affect the heart at multiple levels. In left isomerism, the pulmonary veins from each lung tend to separately enter the posterior wall of the ipsilateral atrium. In both conditions, the hepatic veins may have separate openings in the floor of the atrium or atria, rather than forming a confluence. In a four-chamber view, this strand is seen as a dot in the center of the common atrium (the "central dot sign"), which is pathognomonic for right isomerism.
Syndromes
Additional information:
Usage: a.c.
Tags: 3 mg stromectol buy free shipping, buy discount stromectol 3 mg on-line, stromectol 12 mg order fast delivery, safe 3 mg stromectol
Varek, 56 years: Aseptic meningitis usually occurs in the spring or summer, and enteroviruses are responsible for most cases in children. From time to time, transient depression lasting a few seconds may interrupt the manic activity; this is known as emotional lability.
Zapotek, 65 years: Patients with severe regurgitation can experience heart failure or arrhythmia during pregnancy. These seizures are refractory or only partially responsive to most anticonvulsant drugs.
C-585, Saraswati Vihar, Pitampura, New Delhi 110034





